Abdelrahman Yakout, MD1, William Thomas, MD2, Nikesh Patel, DO2, Imran Khan, MD3 1Mayo Clinic, Gainesville, GA; 2Northeast Georgia Medical Center, Gainesville, GA; 3Northeast Georgia Medical Center, Gainesville, HI Introduction: Small cell carcinoma (SCC) of the pancreas is a very rare neuroendocrine carcinoma characterized by aggressive clinical behavior, early metastasis and poor prognosis. It represents around only 1% of pancreatic malignancies with few cases reported in the literature. We present a case of metastasized SCC of the pancreas, with diagnosis confirmed through a supraclavicular lymph node biopsy.
Case Description/
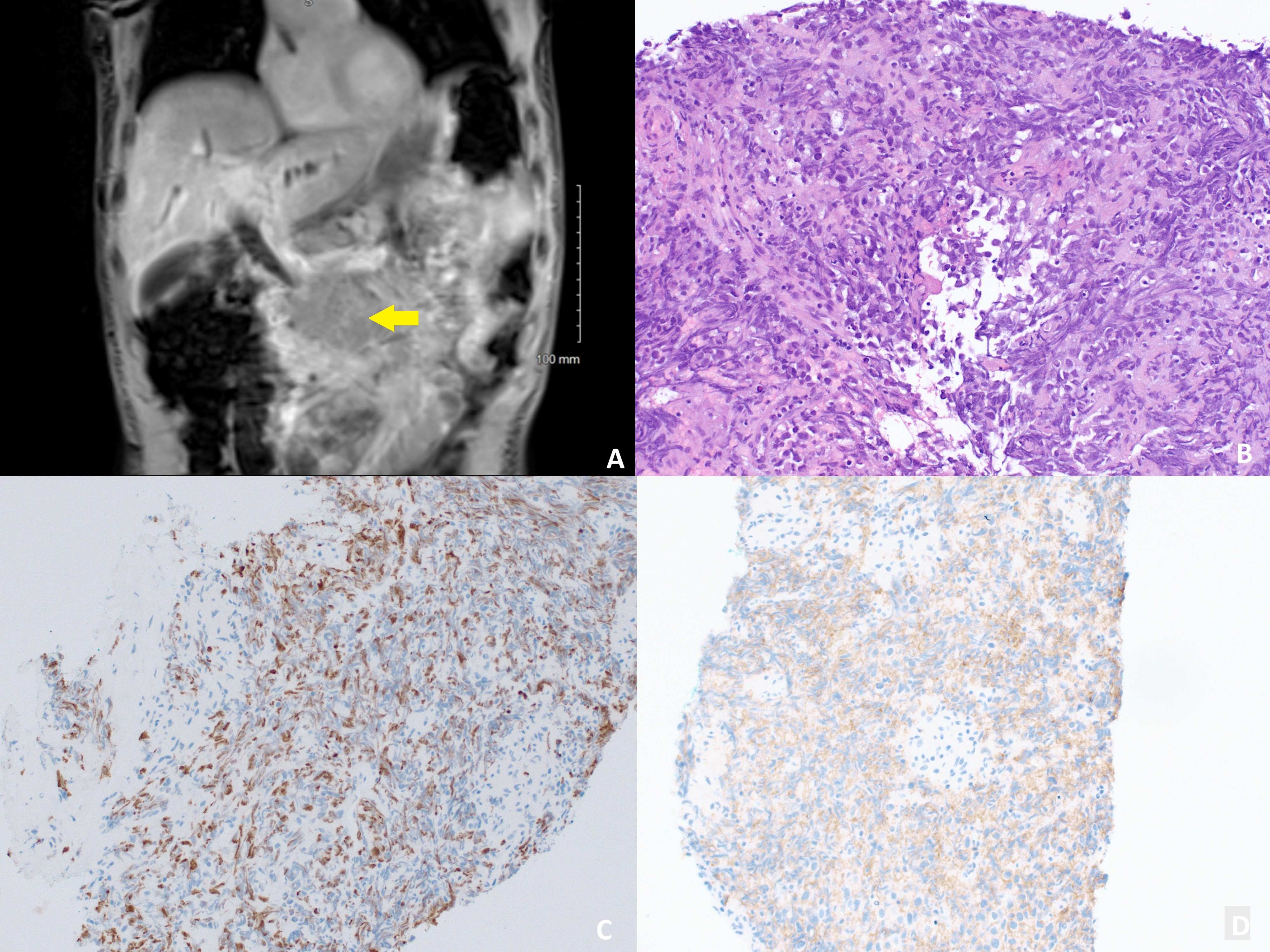
Methods: A 62-year-old man with a 2-year history of smoking, marijuana use, occasional alcohol use presented with epigastric pain radiating to the back for the past 2 weeks, pruritic and profound weight loss over the past 4 months. Labs were notable for total bilirubin of 27.3 mg/dL, AST of 616 U/L, INR of 1.51, and CA 19-9 of 5013 U/mL. CT and MRI with MRCP demonstrated a large, ill-defined mass involving the pancreatic head and body (Figure 1), with biliary duct dilation, retroperitoneal lymphadenopathy, left adrenal mass concerning for metastasis, and supraclavicular lymph node enlargement. CT chest was negative for pulmonary masses. A biliary drain was placed with improvement of his bilirubin and jaundice. Left supraclavicular lymph node biopsy with immunohistochemical staining revealed dot-like positivity in PanKeratin and positive CD56. A Ki-67 showed a proliferation index of >60% (Figure 1). This staining pattern, along with flow cytometry were consistent with metastatic small cell carcinoma. The patient wanted to pursuit treatment with palliative intent. A Gastrojejunostomy was attempted for feeding due to duodenal obstruction by the tumor but was unsuccessful due to adhesions and inability to mobilize the jejunum. A Gastric tube and J- tube were placed alternatively. Despite plans for chemotherapy and radiation, he rapidly decompensated with signs of septic shock requiring pressors. The family decided to transition to comfort care. The patient passed within 2 weeks of his presentation. Discussion: SCC of the pancreas is a rare diagnosis that often presents with widespread metastasis and rapid clinical deterioration. Appropriate management requires tissue confirmation with immunohistochemical workup followed by multidisciplinary intervention
Figure: Figure 1: A. Coronal MRI of the abdomen showing an ill-defined, heterogeneous mass in the pancreatic body and tail (yellow arrow). B. Hematoxylin and eosin (H&E) stained section of supraclavicular lymph node showing small malignant cells with nuclear molding and high proliferation index. C. Ki-67 immunostaining showing a high proliferation index (>60%). D. Immunohistochemical staining for CD56, consistent with neuroendocrine differentiation.
Disclosures: Abdelrahman Yakout indicated no relevant financial relationships. William Thomas indicated no relevant financial relationships. Nikesh Patel indicated no relevant financial relationships. Imran Khan indicated no relevant financial relationships.
Abdelrahman Yakout, MD1, William Thomas, MD2, Nikesh Patel, DO2, Imran Khan, MD3. P0141 - Primary Pancreatic Small Cell Carcinoma: A Rare Entity With Grim Prognosis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.