David Galel, MD1, John Michael Vincent Coralde, MD2, Indraneel Chakrabarty, MD1 1Southwest Healthcare MEC, Temecula, CA; 2Southwest Healthcare MEC, Murrieta, CA Introduction: Laparoscopic cholecystectomy is commonly performed for cases of cholecystitis and other gallbladder pathologies. A key step of this procedure includes ligation of the cystic duct and artery, often using either metallic or plastic polymer surgical clips. There have been prior reported cases of clip migration either intraabdominal or intraductal resulting in various complications, although no clear etiology has objectively been demonstrated thus far.
Case Description/
Methods: A 43-year-old male with history of laparoscopic cholecystectomy 10 years prior complicated by a biliary leak which was stented and a biloma that was drained now in the hospital because of worsening abdominal pain. On his arrival, the patient was tachycardic with low grade fevers, tender to the epigastrium and right upper quadrant. Laboratory values were significant for leukocytosis 23.1k, and transaminitis in cholestatic pattern with total bilirubin increasing from 2.5 to 4.0 in less than 24 hours. Abdominal ultrasound, CT, and MRCP were all consistent with an obstruction of the distal common bile duct. The CT demonstrated a linear object in the distal common bile duct of equal density to a single surgical clip in the gallbladder fossa. We were able to review an abdominal CT from the episode 10 years prior which demonstrated two surgical clips in the gallbladder fossa only. Broad spectrum antibiotics were initiated due to concern for cholangitis. ERCP was performed with successful removal of obstructing object, which consisted of an intact metal surgical clip with a small amount biliary sludge. The patient subsequently recovered as expected and was discharged without complication. Discussion: Multiple occurrences of surgical clip migration have been reported following laparoscopic cholecystectomy. It has been documented with both metal and plastic clips, at highly variable intervals ranging from a few months to several decades, and without a clear etiology. Several theories of this phenomenon have been proposed including concurrent inflammatory process during placement or even poor surgical technique. Given the presentation of our case in conjunction with prior case studies, we believe that either bile leak and/or regional inflammation are likely the most significant risk factors. Though this phenomenon appears to be rare overall, due to its repeated occurrences and potential for further morbidity clip migration should certainly be on the differential for a patient with biliary obstruction post-cholecystectomy.
Figure: Coronal view of CT abdomen demonstrating linear hyperdense object in the distal common bile duct (yellow arrow) of equal density to a single metallic clip in the gallbladder fossa (not pictured).
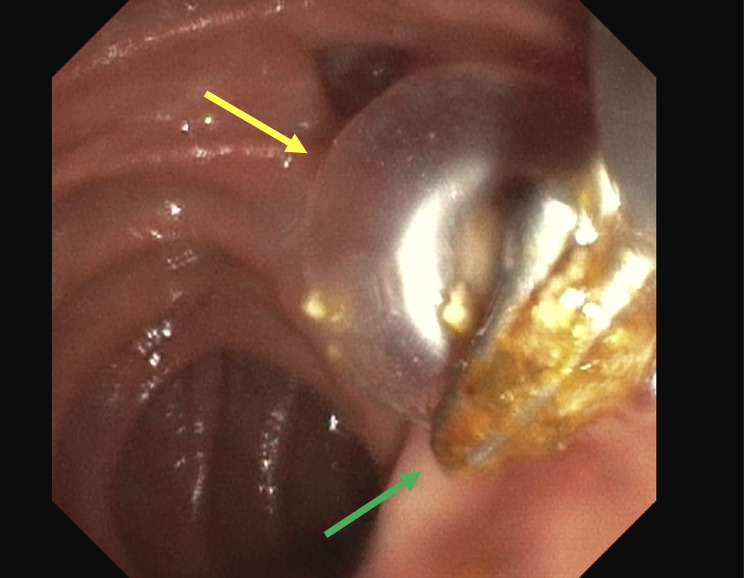
Figure: Intraluminal view of the duodenum during ERCP demonstrating sweeping balloon (yellow arrow) and metal clip (green arrow).
Disclosures: David Galel indicated no relevant financial relationships. John Michael Vincent Coralde indicated no relevant financial relationships. Indraneel Chakrabarty indicated no relevant financial relationships.
David Galel, MD1, John Michael Vincent Coralde, MD2, Indraneel Chakrabarty, MD1. P0099 - Post-Cholecystectomy Clip Migration Resulting in Biliary Obstruction: A Rare but Important Complication, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")