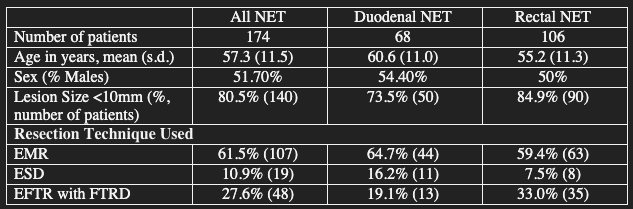
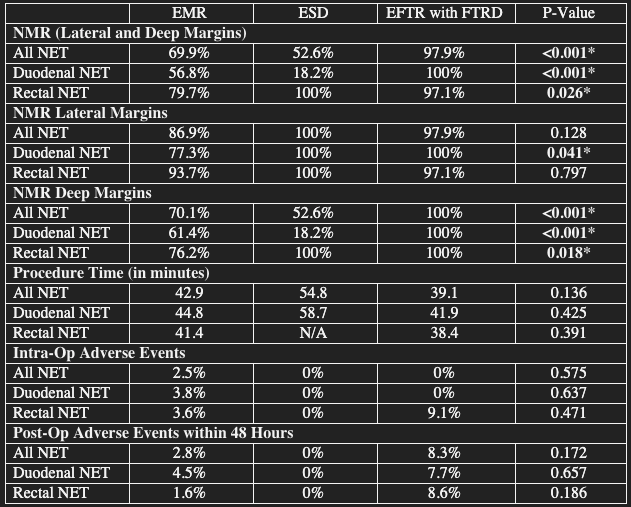
Joy Zhao, MD1, Adam Goodman, MD2, Sunil Dacha, MD3, Elizza Villarruel, 4, Danny Issa, MD5, Ravishankar Asokkumar, MBBS6, Abdulrahman Qatomah, MBBS7, Daryl Ramai, MD, MPH, MSc8, Hiroyuki Aihara, MD, PhD7, Harneet Sangha, BS9, Mohit Girotra, MD10, Haidar Khan, MD11, Daniel Kurtz, DO11, Rashmi Advani, MD11, Anuroop Yekula, MBBS12, Vivek Kaul, MD, FACG13, Shivangi Kothari, MD, FACG12, Truptesh H. Kothari, MD, MS, FACG13, Anand Kumar, MD, MPH14 1Thomas Jefferson University, Philadelphia, PA; 2NYU Grossman School of Medicine, Division of Gastroenterology and Hepatology, New York, NY; 3Houston Methodist Hospital, Houston, TX; 4David Geffen School of Medicine at UCLA, Los Angeles, CA; 5David Geffen School of Medicine at UCLA, West Hills, CA; 6Singapore General Hospital, N/A, Singapore; 7Brigham and Women's Hospital, Boston, MA; 8Brigham and Women’s Hospital, Harvard Medical School, Salt Lake City, UT; 9Washington State University Elson S. Floyd School of Medicine, Spokane, WA; 10Swedish First Hill Medical, Seattle, WA; 11Mount Sinai South Nassau,Icahn School of Medicine at Mount Sinai, Oceanside, NY; 12University of Rochester, Rochester, NY; 13University of Rochester Medical Center, Rochester, NY; 14Thomas Jefferson University Hospital, Philadelphia, PA Introduction: Endoscopic resection is recommended for localized duodenal and small rectal neuroendocrine tumors (NET). Endoscopic mucosal resection (EMR), endoscopic submucosal dissection (ESD), and endoscopic full-thickness resection (EFTR) using full-thickness resection device (FTRD) have been used with varying success. A direct comparison of these techniques has not been performed thus far. Our aim is to compare clinical outcomes of rectal and duodenal NET resection via EMR, ESD and EFTR with FTRD. Methods: A retrospective multicenter study (9 centers) was performed, including patients >18 years old with diagnosis of duodenal or rectal NET, and have NET resection by EMR, ESD, or EFTR between 2016 and 2025. NET >2 cm and positive lymph nodes or distant metastases where endoscopic resection is not indicated were excluded. Primary outcomes were negative margin rate (NMR) for deep and lateral margins, procedure time, and adverse events. Comparison groups were based on resection type and/or NET location. Statistical analyses were performed with SPSS with P-value < 0.05 indicating statistical significance. Results: 174 patients with NET (68 duodenal, 106 rectal) were included. Mean age was 57.3 years with 51.7% males (Table 1). Over 80% of the NET (73.5% duodenum, 84.9% rectum) were <10mm. EMR was the most common resection method (61.5% all NET, 64.7% duodenum, 59.4% rectum). NMR for lateral and deep margins was significantly higher in the EFTR with FTRD group compared to EMR and ESD (97.9% EFTR vs 69.9% EMR and 52.6% ESD; p< 0.001). ESD for duodenal NET had the lowest NMR for deep margins at 18.2%. Adverse events were not significantly different between the three groups (Table 2). Discussion: For small (<20 mm) duodenal and rectal NET, EFTR with FTRD offers the best chance of R0 resection due to higher NMR for deep and lateral margins. EFTR with FTRD also has favorable procedure times and similar adverse events compared to EMR and ESD. Prospective comparative studies are needed to validate these findings.
Figure: Table 1. Demographic Data and Characteristics
Figure: Table 2. Outcomes of Interest Based on Resection Technique *P-Value <0.05 considered significant.
Disclosures: Joy Zhao indicated no relevant financial relationships. Adam Goodman: Ambu, Inc – Advisor or Review Panel Member. Boston Scientific – Advisor or Review Panel Member. Iterative Health – Advisor or Review Panel Member. Sunil Dacha indicated no relevant financial relationships. Elizza Villarruel indicated no relevant financial relationships. Danny Issa: Boston Scientific – Consultant. Ravishankar Asokkumar indicated no relevant financial relationships. Abdulrahman Qatomah indicated no relevant financial relationships. Daryl Ramai indicated no relevant financial relationships. Hiroyuki Aihara indicated no relevant financial relationships. Harneet Sangha indicated no relevant financial relationships. Mohit Girotra indicated no relevant financial relationships. Haidar Khan indicated no relevant financial relationships. Daniel Kurtz indicated no relevant financial relationships. Rashmi Advani indicated no relevant financial relationships. Anuroop Yekula indicated no relevant financial relationships. Vivek Kaul indicated no relevant financial relationships. Shivangi Kothari indicated no relevant financial relationships. Truptesh Kothari indicated no relevant financial relationships. Anand Kumar: Boston Scientific – Consultant. Olympus – Consultant. Pentax – Paid Speaker.
Joy Zhao, MD1, Adam Goodman, MD2, Sunil Dacha, MD3, Elizza Villarruel, 4, Danny Issa, MD5, Ravishankar Asokkumar, MBBS6, Abdulrahman Qatomah, MBBS7, Daryl Ramai, MD, MPH, MSc8, Hiroyuki Aihara, MD, PhD7, Harneet Sangha, BS9, Mohit Girotra, MD10, Haidar Khan, MD11, Daniel Kurtz, DO11, Rashmi Advani, MD11, Anuroop Yekula, MBBS12, Vivek Kaul, MD, FACG13, Shivangi Kothari, MD, FACG12, Truptesh H. Kothari, MD, MS, FACG13, Anand Kumar, MD, MPH14, 3, Comparison of EMR, ESD, and EFTR for Endoscopic Resection of Duodenal and Rectal Neuroendocrine Tumors, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.