70 - Efficacy and Safety of Subcutaneous Guselkumab Rescue Therapy in Patients With Moderately to Severely Active Crohn’s Disease and Inadequate Response to Ustekinumab: Results From GALAXI 1, 2, & 3 Long-Term Extension
Anita Afzali, MD, MPH, MHCM, FACG1, Douglas Wolf, MD2, Rupert Leong, MBBS, MD, FRACP3, Rian Van Rampelbergh, MD4, Wilbert van Duijnhoven, MSc4, Christopher Busse, MS5, Tadakazu Hisamatsu, MD, PhD6, Julián Panés, MD7 1University of Cincinnati College of Medicine, Cincinnati, OH; 2Atlanta Gastroenterology Associates, Atlanta, GA; 3Macquarie University Hospital, Sydney, New South Wales, Australia; 4Johnson & Johnson, Antwerp, Antwerpen, Belgium; 5Johnson & Johnson, Horsham, PA; 6Kyorin University School of Medicine, Tokyo, Tokyo, Japan; 7Hospital Clínic de Barcelona, IDIBAPS, CIBERehd, Barcelona, Catalonia, Spain Introduction: The phase 2b GALAXI 1 and phase 3 GALAXI 2&3 studies evaluated guselkumab(GUS), a dual-acting IL-23p19 subunit inhibitor, in pts with moderately to severely active CD. Pts treated with ustekinumab(UST) who met inadequate response criteria during the long-term extension(LTE) could switch to GUS 200mg SC q4w. We present efficacy/safety results in pts who received GUS after experiencing an inadequate response to UST in the pooled GALAXI LTE. Methods: Individuals with prior inadequate response/intolerance to UST were excluded from GALAXI; however, during the LTE, pts treated with UST 90mg SC q8w who met inadequate treatment response criteria(not in clinical response and CDAI ≥220) between Wks52-80 were eligible for treatment switch to GUS 200mg SC q4w, without IV induction. Clinical response and clinical remission were both assessed 16wks after treatment switch. Endoscopic response and endoscopic remission were assessed at Wk96(definitions in Figure). Safety was assessed through Wk96. Results: In total, 80 pts treated with UST underwent treatment switch to GUS 200mg SC q4w;75 pts were included in the efficacy analyses(baseline mean age, 35.2yrs; male, 64.0%; mean CD disease duration, 8.21yrs; mean CDAI, 291.5; mean SES-CD, 12.8; history of inadequate response/intolerance to biologics[BIO-IR], 60.0%).
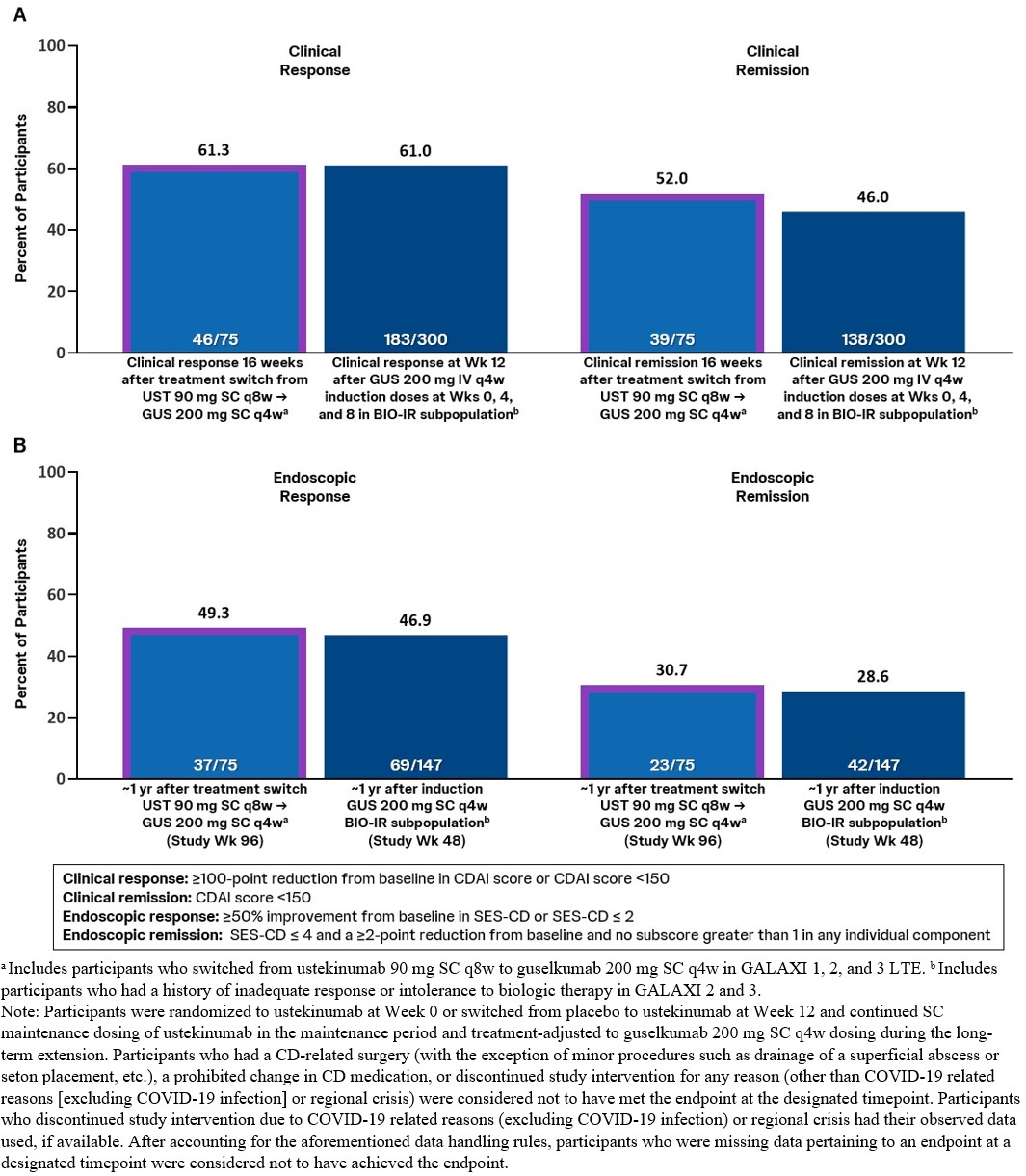
Proportions of pts achieving clinical response and clinical remission 16wks after treatment switch from UST to GUS 200mg SC q4w were comparable to proportions of pts treated with GUS 200mg IV q4w induction in the pooled GALAXI 2&3 BIO-IR subgroup who achieved clinical response and clinical remission at Wk12(Figure).
Proportions of pts achieving endoscopic response and endoscopic remission at Wk96(ie, ~1yr after treatment switch) were similar to proportions of pts in the pooled GALAXI 2&3 BIO-IR subgroup receiving GUS 200mg SC q4w maintenance who achieved endoscopic response and endoscopic remission at Wk48.
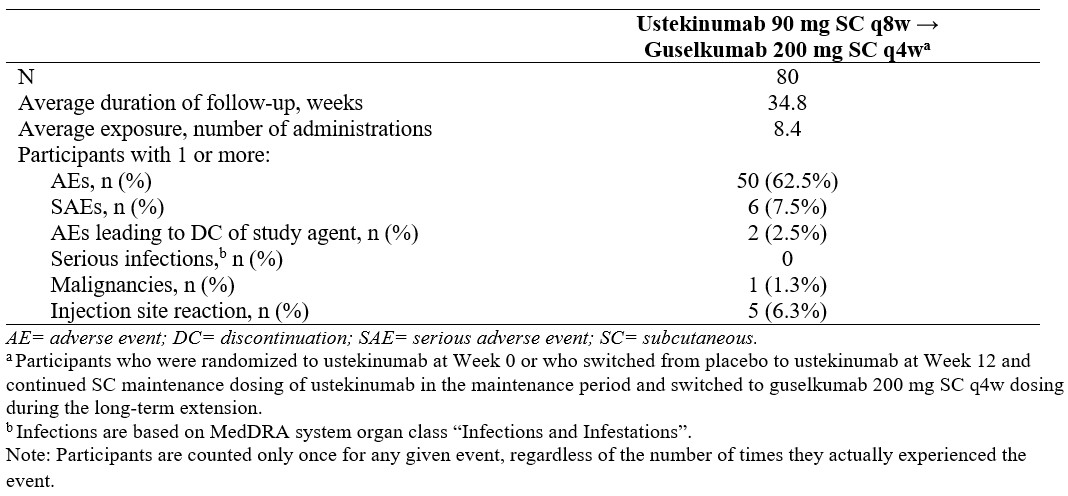
Safety results are summarized in the Table. Discussion: Among pts who experienced inadequate response to UST in the LTE, more than half achieved clinical remission 16wks after treatment switch to GUS 200mg SC q4w, and ~50% were in endoscopic response ~1yr after treatment switch. These data suggest pts with an inadequate treatment response to UST may benefit from GUS treatment. Results should be interpreted considering that pts received GUS SC maintenance therapy directly without IV induction. Key safety event rates were consistent with the known safety profile of GUS in approved indications.
Figure: Figure. Clinical Outcomes 16 Weeks After Treatment Switch (A), and Endoscopic Outcomes at Study Week 96 (B)
Figure: Table. Safety Summary From Treatment Switch Through Week 96
Anita Afzali, MD, MPH, MHCM, FACG1, Douglas Wolf, MD2, Rupert Leong, MBBS, MD, FRACP3, Rian Van Rampelbergh, MD4, Wilbert van Duijnhoven, MSc4, Christopher Busse, MS5, Tadakazu Hisamatsu, MD, PhD6, Julián Panés, MD7, 70, Efficacy and Safety of Subcutaneous Guselkumab Rescue Therapy in Patients With Moderately to Severely Active Crohn’s Disease and Inadequate Response to Ustekinumab: Results From GALAXI 1, 2, & 3 Long-Term Extension, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.