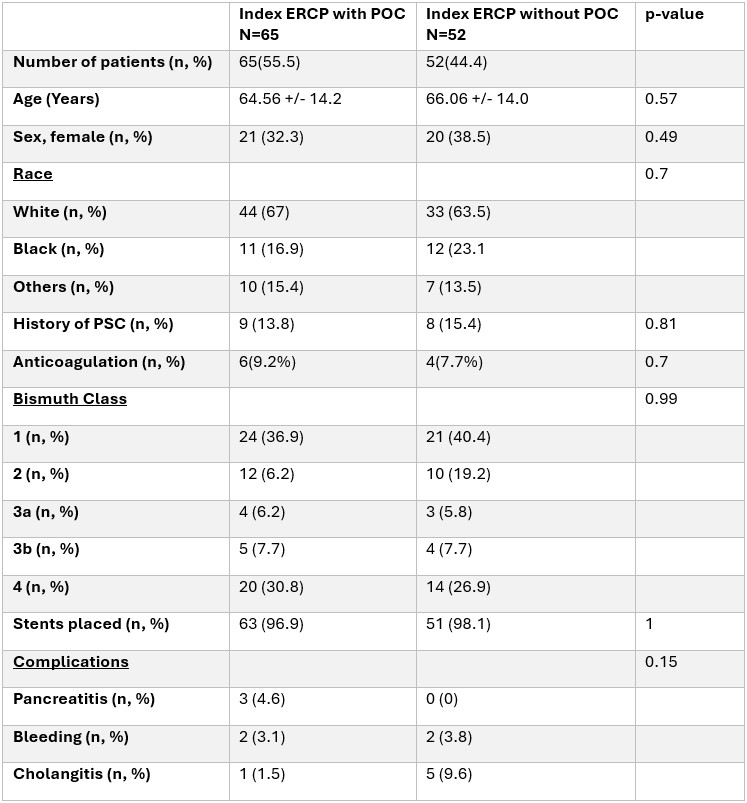
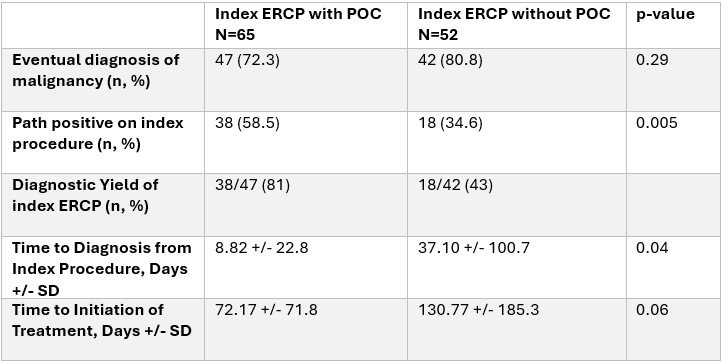
Muhammad Saad Faisal, MD1, Jonathan A. Montrose, DO1, Muhammad Salman Faisal, MD2, Ammad Javaid. Chaudhary, MD1, Sumit Singla, MD1 1Henry Ford Health, Detroit, MI; 2Henry Ford Hospital, Detroit, MI Introduction: Indeterminate hilar biliary strictures present a diagnostic and management challenge, with no established guidelines. Endoscopic Retrograde Cholangiopancreatography (ERCP) is used for sampling and management of these strictures, however, the low yield of ERCP may delay diagnosis and treatment. Per Oral Cholangioscopy (POC) offers direct visualization of the biliary tree and allows for targeted biopsies. However, concerns exist about the increased adverse events (AEs) with increased instrumentation during the index procedure. We aim to assess the safety, efficacy, and AE profile of POC used in index ERCP for the diagnosis and management of hilar strictures compared to standard ERCP. Methods: We conducted a retrospective cohort study of patients who underwent ERCP for indeterminate hilar strictures from 2018–2024 across a multicenter system. Patients were divided into two groups based on POC use during index ERCP. Primary outcome was time to diagnosis; secondary outcomes included time to treatment and AEs (cholangitis, sepsis, bacteremia, pancreatitis). Results: Among 117 patients meeting our inclusion criteria, 65 (55.5%) underwent ERCP with POC (case group), and 52 (44.4%) underwent standard ERCP (control group). No significant differences in age, gender, ethnicities, PSC, anticoagulation use, and Bismuth classifications were found. Stents were placed in 96.9% (case) vs. 98.1% (control) (p=1). Adverse events were not significantly different: pancreatitis (4.6% vs. 0%), bleeding (3.1% vs. 3.8%), cholangitis (1.5% vs. 9.6%). In the case group, 87% had biliary sampling with brushing and cholangioscopy-directed biopsies, 6.5% with intraductal forceps, and 6.5% with brushings alone. In the control group, 71% had brushings alone and 29% had brushings along with intraductal forceps biopsy. Malignancy was diagnosed in 72.3% (case) vs. 80.8% (control). Pathology confirmed malignancy in 58.5% (case) vs. 34.6% (control) (p=0.005). Diagnostic yield of index ERCP was 81% in the case group compared to 43% in the control group. Mean time to diagnosis was significantly shorter in the case group (8.82 ± 22.8 days vs. 37.10 ± 100.7; p=0.04). Time to treatment initiation trended shorter (72.17 ± 71.8 vs. 130.77 ± 185.3 days; p=0.06). Discussion: For patients with indeterminate hilar biliary strictures, POC used during index ERCP increased diagnostic yield, shortened the time to establishment of diagnosis, and does not have increased adverse events compared to standard ERCP during index procedure.
Figure: Table 1. Summary of patient and procedural characteristics.
Figure: Table 2. Summary of diagnostic characteristics
Disclosures: Muhammad Saad Faisal indicated no relevant financial relationships. Jonathan Montrose indicated no relevant financial relationships. Muhammad Salman Faisal indicated no relevant financial relationships. Ammad Chaudhary indicated no relevant financial relationships. Sumit Singla: Boston Scientific. – Consultant.
Muhammad Saad Faisal, MD1, Jonathan A. Montrose, DO1, Muhammad Salman Faisal, MD2, Ammad Javaid. Chaudhary, MD1, Sumit Singla, MD1, 59, Safety and Efficacy of Per Oral Cholangioscopy (POC) in Index ERCP for Patients With Indeterminate Hilar Strictures, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.



 photo")