65 - Efficacy and Safety of Icotrokinra, a Targeted Oral Peptide That Selectively Blocks IL-23 Receptor Activation, in Ulcerative Colitis: Results From Week 28 of ANTHEM-UC, a Phase 2b Dose-Ranging Trial
Vipul Jairath, MBChB, DPhil, MRCP1, Britta Siegmund, MD2, Lindsey Surace, MD3, Ngozi Erondu, MD, PhD3, Minhu Chen, MD, PhD4, Karen Chachu, MD, PhD5, Edouard Louis, MD, PhD6, Katsuyoshi Matsuoka, MD, PhD7, Jimmy Limdi, MD8, Edmund Arthur, PharmD, MBA3, Nicole Houck, BS3, Mary Ellen Frustaci, BS, MS3, Joyce Zhan, PhD3, Grazyna Rydzewska, MD, PhD9, Edward V.. Loftus, MD10, Maria T.. Abreu, MD11 1Western University, London, ON, Canada; 2Charité – Universitätsmedizin Berlin, corporate member of Freie Universität Berlin and Humboldt-Universität zu Berlin, Berlin, Berlin, Germany; 3Johnson & Johnson, Spring House, PA; 4The First Affiliated Hospital, Sun Yat-sen University, Guangzhou, Guangdong, China; 5Duke University School of Medicine, Durham, NC; 6CHU Liège University Hospital, Liège, Liege, Belgium; 7Toho University Sakura Medical Center, Chiba, Chiba, Japan; 8Northern Care Alliance NHS Foundation Trust and University of Manchester, Manchester, England, United Kingdom; 9National Medical Institute of Ministry of Interior and Administration, Warsaw, Mazowieckie, Poland; 10Mayo Clinic College of Medicine and Science and Mayo Clinic, Rochester, MN; 11Cedars-Sinai, Los Angeles, CA Introduction: As previously reported, all 3 doses of icotrokinra (ICO; JNJ-2113) — a first-in-class targeted oral peptide that selectively blocks IL-23 receptor activation — met the week (W) 12 primary endpoint in ANTHEM-UC, a Phase 2b, randomized, double-blind, placebo-controlled, treat-through, dose-ranging study in adults with moderate to severe ulcerative colitis (UC). Here we report W28 efficacy and safety of ICO from ANTHEM-UC. Methods: Participants (pts) had a modified Mayo score (mMS) of 5–9 inclusive, a Mayo endoscopy subscore (MES) ≥2, and inadequate response/intolerance (IR) to TNFα blockers, vedolizumab, ustekinumab, JAK inhibitors, or S1P receptor modulators (BIO/JAKi/S1P-IR) or IR to corticosteroids, AZA, or 6-MP. Randomization (1:1:1:1) to once-daily (qd) oral ICO 100 mg, 200 mg, 400 mg or placebo (PBO) was stratified by BIO/JAKi/S1P-IR status (Y/N) and MES (2 or 3).
Clinical response at W12 was the primary endpoint. Clinical response, clinical remission, symptomatic remission, endoscopic improvement, and histologic-endoscopic mucosal improvement (HEMI) were further evaluated at W28 as exploratory endpoints. Pts meeting inadequate response criteria at W16 had a treatment adjustment: PBO pts switched to ICO 400 mg qd and ICO pts had a sham adjustment. All pts meeting inadequate response criteria were considered non-responders moving forward. Results: Analyses included all 252 randomized pts who received study medication: mean mMS, 6.63; mMS >7, 31.9%; MES=3, 58.7%; BIO/JAKi/S1P-IR, 43.3%. W16 inadequate response criteria were met by 24 (38.1%), 11 (17.2%), 11 (17.7%) and 7 (11.1%) pts receiving PBO & ICO 100, 200 and 400 mg.
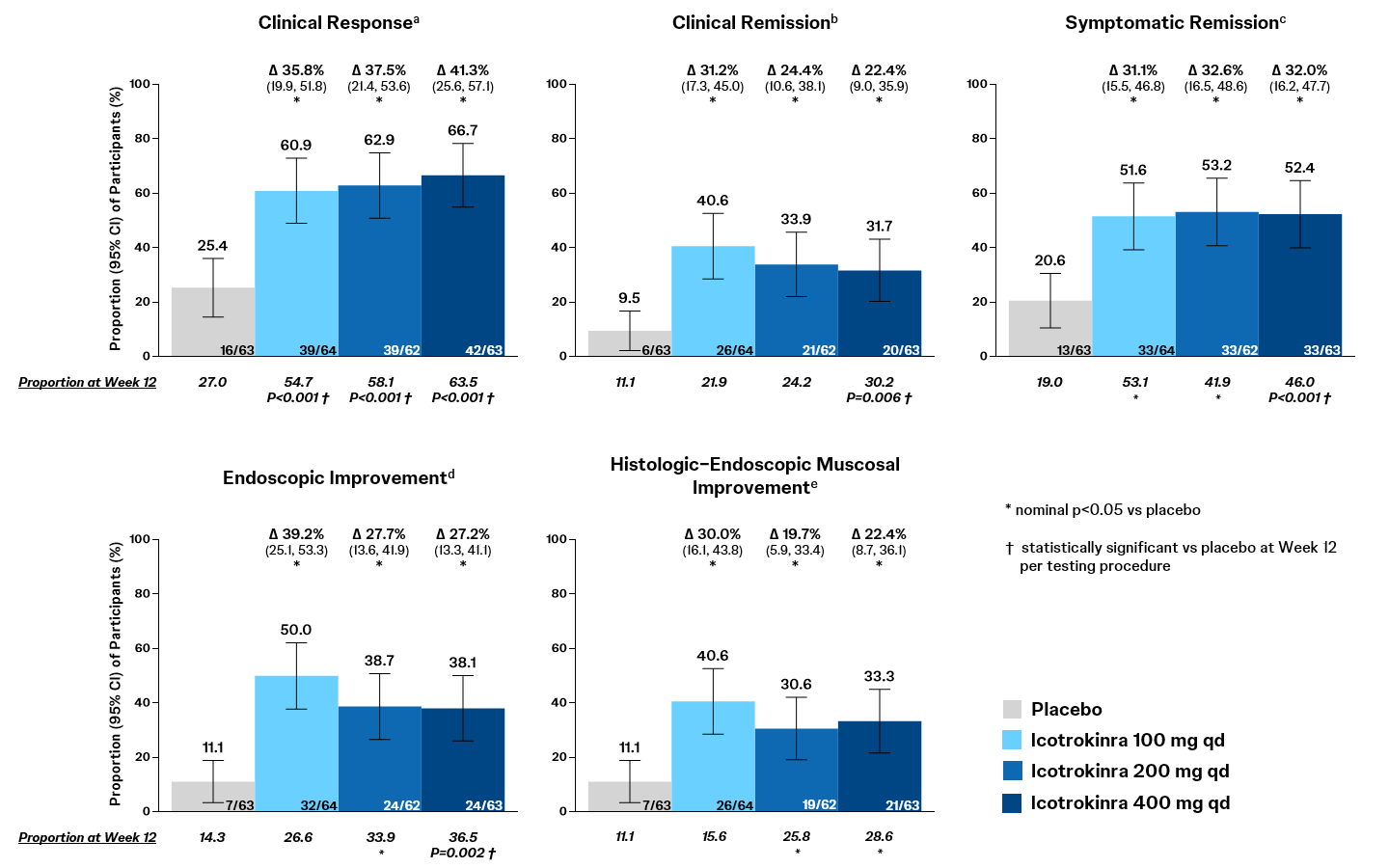
Relative to PBO, all ICO doses demonstrated clinically meaningful rates of clinical response, clinical remission, symptomatic remission, endoscopic improvement, and HEMI at W28 (Figure). Relative to W12 outcomes, rates of clinical response, clinical remission, endoscopic improvement, and HEMI continued to increase through W28 in each ICO dose group.
Through W28, ≥1 AE (61.9%, 65.6%, 66.1%, 60.3%), SAEs (9.5%, 0%, 4.8%, 1.6%), or AEs leading to discontinuation of study agent (11.1%, 0%, 6.5%, 3.2%) were reported in pts in the PBO & ICO 100, 200 and 400 mg groups. No serious or opportunistic infections, tuberculosis, malignancies, clinically important hepatic disorders, VTE, MACE, or deaths were reported with ICO. Discussion: In ANTHEM-UC, clinical efficacy and a favorable safety profile were observed with once-daily ICO through W28 in pts with moderate to severe UC.
Figure: Week 28 Outcomes in ANTHEM-UC: Data presented as percentage of participants attaining the endpoint, with adjusted treatment difference (Δ), 95% confidence interval (CI) for the adjusted treatment difference, and p-value versus placebo. At Week 28, all endpoints are exploratory and p-values are nominal. Outcomes at Week 12 that reached statistical significance per the prespecified testing procedure are indicated. Adjusted treatment differences, 95% CIs, and p-values were based on the common risk difference by use of Mantel-Haenszel stratum weights and the Sato variance estimator, using stratification factors of inadequate response/intolerance to TNF blockers, vedolizumab, ustekinumab, JAK inhibitors, or S1P receptor modulators (Yes or No) and Mayo endoscopy subscore (MES) (2 [moderate] or 3 [severe]). Participants with intercurrent events of ostomy or colectomy, prohibited changes in UC medication, discontinuation of study intervention for any reason except those due to major disruptions (e.g., COVID-19 related reasons or regional crisis, excluding COVID-19 infection), or meeting Week 16 inadequate response criteria were considered nonresponders for the Week 28 endpoints, as were participants who had missing data for the endpoint.
ENDPOINT DEFINITIONS: a. Clinical response: a decrease from baseline in modified Mayo score by ≥30% and ≥2 points with either a ≥1-point decrease from baseline in rectal bleeding subscore or a rectal bleeding subscore of 0 or 1. b. Clinical remission: stool frequency subscore of 0 or 1, rectal bleeding subscore of 0, and MES of 0 or 1. c. Symptomatic remission: stool frequency subscore of 0 or 1 and rectal bleeding subscore of 0 d. Endoscopic improvement: MES of 0 or 1. e. Histologic-endoscopic mucosal improvement (HEMI): histologic remission (absence of neutrophils from the mucosa [both lamina propria and epithelium], no crypt destruction, and no erosions, ulcerations, or granulation tissue according to the Geboes grading system) AND endoscopic improvement (MES of 0 or 1).