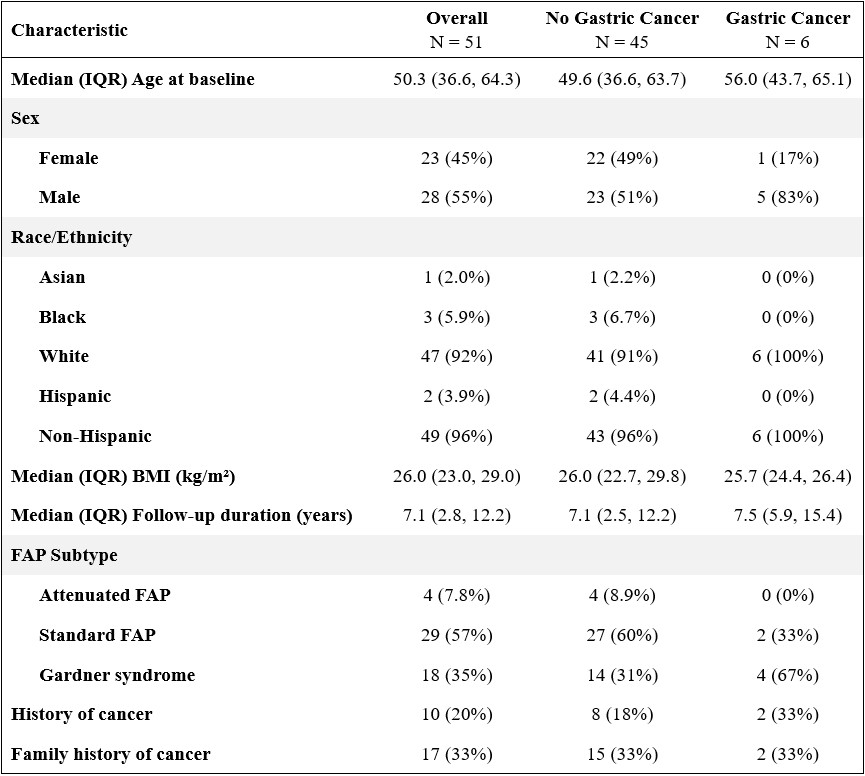
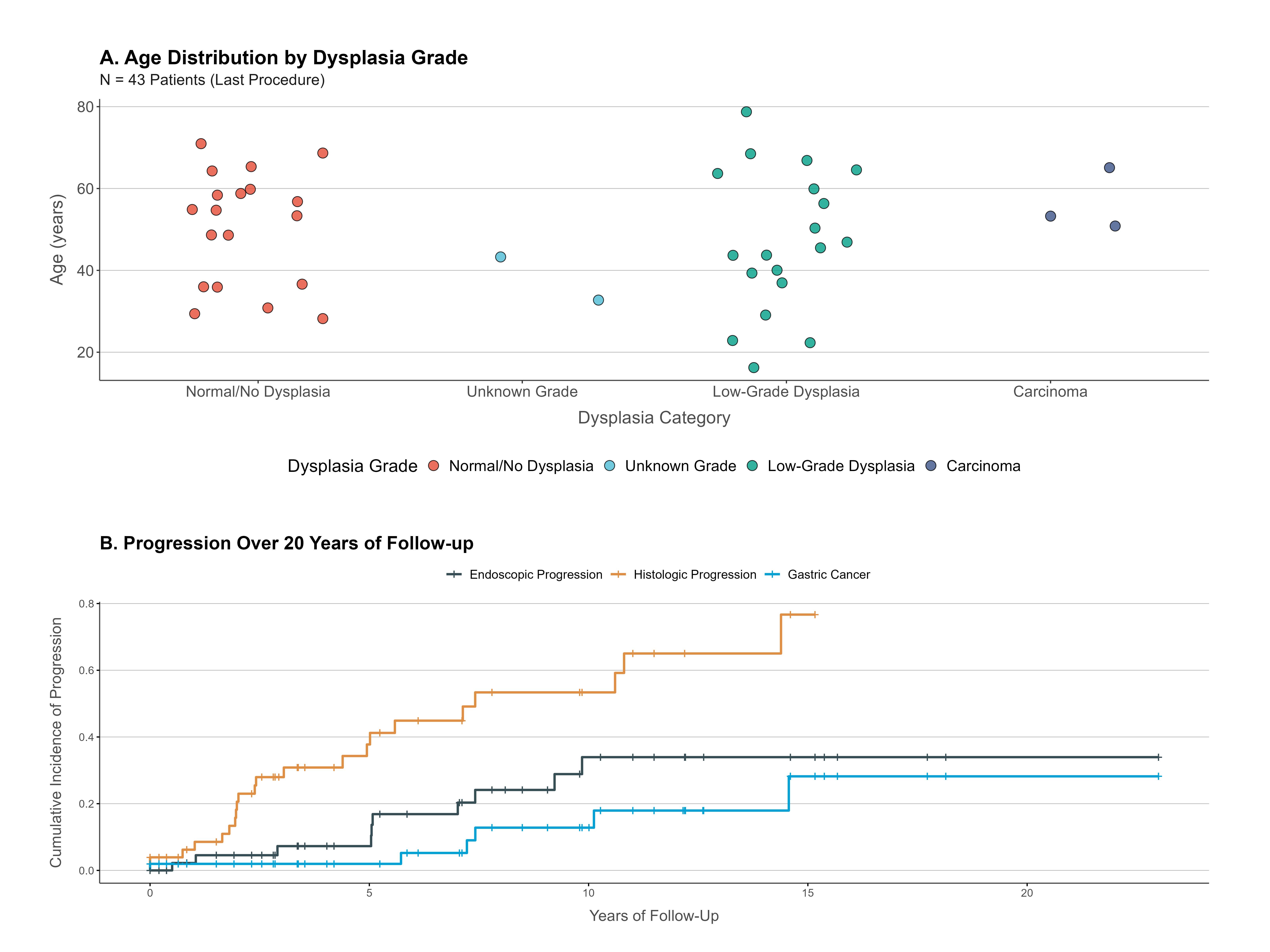
Yun Wang, MD1, Malak Munir, MD1, Kenneth Park, MD1, Laith H. Jamil, MD, FACG2, Srinivas Gaddam, MD, MPH1, Simon K.. Lo, MD, FACG1 1Cedars-Sinai Medical Center, Los Angeles, CA; 2Corewell Health William Beaumont University Hospital Gastroenterology, Royal Oak, MI Introduction: Familial adenomatous polyposis (FAP) is caused by germline APC mutations. Second to colorectal cancer, duodenal cancer (DC) is the leading cause of death, prompting upper endoscopic surveillance. However, fundic gland polyps (FGPs) have poorly defined malignant potential with reported gastric cancer (GC) risk of 2-4%. Evidence-based strategies for surveillance of upper GI malignancies in FAP are lacking. Methods: We conducted a retrospective cohort study of FAP patients undergoing endoscopic fundic gland polypectomy surveillance (2001-2025). Endoscopic progression was defined as increases in polyp size/number/distribution; histologic progression as advancement from normal to dysplasia/carcinoma. Kaplan-Meier estimates were used to calculate 10-year cumulative incidence. Associations were assessed using generalized linear regression models. Results: 51 FAP patients (mean age 52.6±16.7 years, 45.1% female, 92.2% white) were followed for median 84.6 months. 6 (11.8%) developed GC at mean age 52.5±14.5 years. No DC occurred despite 66.7% having duodenal/ampullary polyps (11 patients with Spiegelman Score III/IV). Mean age at first dysplasia detection was 44±14.8 years. Overall, 52.9% had low-grade dysplasia, while 3.9% had high-grade dysplasia. Of 25 patients without initial dysplasia, 16 progressed histologically. GC development followed dysplasia-carcinoma sequence in 4 patients. Among patients with serial FGP biopsies, 43.1% had histologic progression with 10-year cumulative incidence 53.4% (95% CI 31.7-68.1). In GC patients, 83.3% had preceding FGP dysplasia, while 33.3% had pyloric gland adenomas. Polyp size ≥1cm was strongly associated with cancer (P < 0.01). Endoscopic progression was less common (19.6%), with 10-year cumulative incidence 33.9% (95% CI 13-49.9). However, only endoscopic progression was significantly associated with GC (P < 0.01). Discussion: Contrary to conventional belief, GC occurred at surprisingly high risk in our cohort. Despite 66.7% having duodenal polyps (11 with a high Spiegelman score), we encountered no DC, possibly attributable to effective snare polypectomy. Our findings support endoscopic FGP surveillance starting at age 45 and therapeutic removal of FGP ≥1cm. However, large collaborative studies are needed to establish evidence-based prevention strategies for this high-risk population.
Figure: Table 1. Baseline Characteristics of FAP Patients
Figure: Figure 2. (A) Distribution of Age by Dysplasia Grade at Most Recent Endoscopy; (B) Cumulative Incidence of Progression Over 20 Years of Follow-Up
Disclosures: Yun Wang indicated no relevant financial relationships. Malak Munir indicated no relevant financial relationships. Kenneth Park indicated no relevant financial relationships. Laith Jamil indicated no relevant financial relationships. Srinivas Gaddam indicated no relevant financial relationships. Simon Lo indicated no relevant financial relationships.
Yun Wang, MD1, Malak Munir, MD1, Kenneth Park, MD1, Laith H. Jamil, MD, FACG2, Srinivas Gaddam, MD, MPH1, Simon K.. Lo, MD, FACG1, 48, Fundic Gland Polyp Outcomes in Familial Adenomatous Polyposis: A Long-Term Follow-Up Study, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.