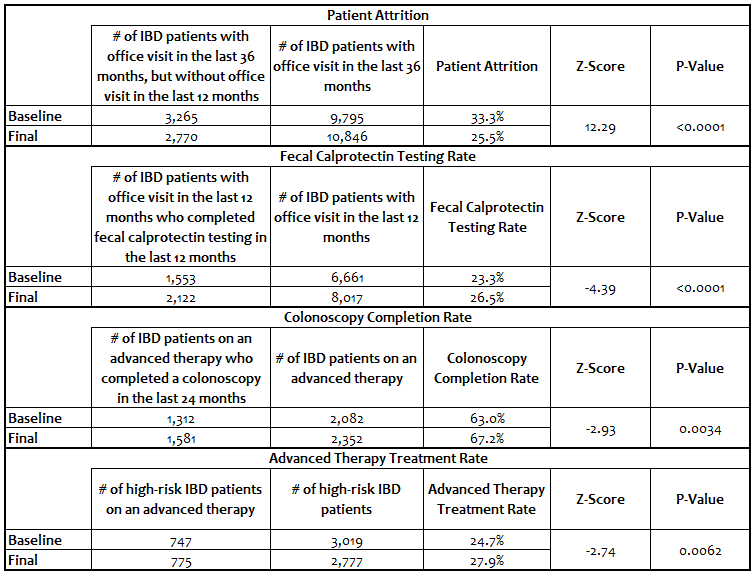
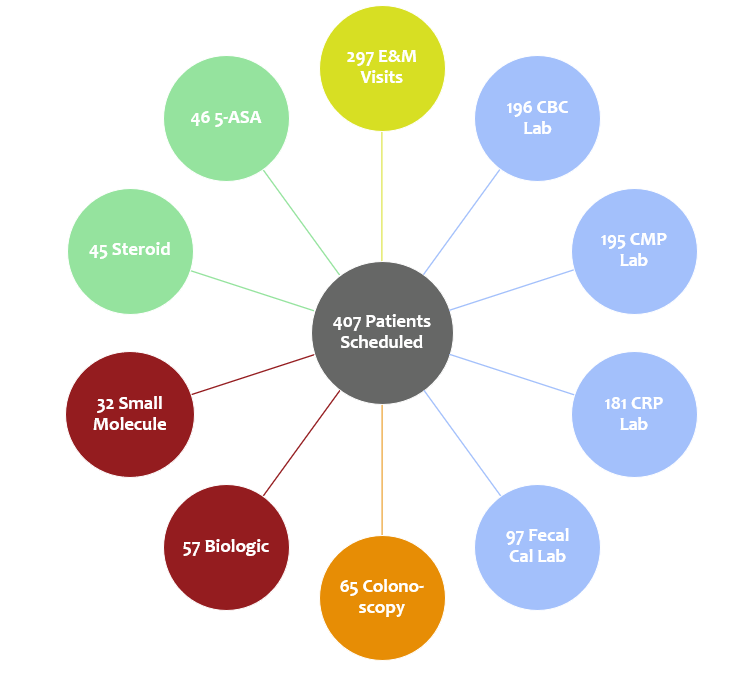
Michael Mills, MD, MPH, FACG1, Gena Ettinger, PA-C, MSHS2, Nicole Smith, BS, MS3, Wanda L.. Wilt, 4, Paul Berggreen, MD5 1University of Arizona/Arizona Digestive Health/GI Alliance, Phoenix, AZ; 2GI Alliance, Roanoke, TX; 3Specialty Networks/Cardinal Health, Powell, OH; 4Specialty Networks/Cardinal Health, Columbus, OH; 5GI Alliance, Phoenix, AZ Introduction: Effective IBD management requires close clinical and laboratory monitoring with proactive treatment adjustments. Despite published guidelines, variability in care highlights the need for data-driven approaches to assess and improve adherence. We leveraged a novel actionable data-fed IBD Dashboard to assess practice performance in real time and measured success over a 6-month pilot with 9,795 active IBD patients in six community-based GI practices across four states. Methods: Six key performance indicators (KPIs) aligned with evidence-based treat-to-target STRIDE-II recommendations were chosen by a key opinion leader group. Our primary aim was to use a novel IBD Dashboard to improve KPI adherence. KPIs measured annual patient attrition rate, annual laboratory protocol adherence, colonoscopy completion rate every two years for those on advanced therapy, advanced therapy use in high-risk patients, prescription patterns of mesalamine for Crohn’s disease, and enrollment in chronic care management. Six sites were chosen from 144 locations, with each site selecting a champion to implement and oversee the pilot. Staff were trained to use the Dashboard consistently, and monthly meetings addressed current performance, identification of barriers, and workflow adjustments. A two-proportion z-test was used for statistical analysis of aggregated data for comparison of baseline to conclusion of pilot. Results: Significant improvement across multiple metrics were identified, including a reduction in patient attrition from 33% to 26% (p < 0.0001); lab testing rate increased from 23% to 26% (p < 0.0001); colonoscopy completion rate rose from 63% to 67% (p = 0.003); and advanced therapy treatment rate increased from 25% to 28% (p = 0.006) (Table 1). Through patient identification, 407 patients that had failed to follow up were scheduled for an office visit. At pilot conclusion, 297 completed the scheduled office visit; of these, 65 had a colonoscopy, 57 were started or switched to a biologic, and 32 on a small molecule (Figure 1). Discussion: This pilot is the first IBD Dashboard initiative with in-progress expansion across a 22-state, community-based GI practice. Unlike prior efforts confined to single sites or regional centers, this project demonstrates scalable improvement in IBD care. Care processes are now proactive and standard at all six sites and are expanding into other disease states. Future AI integration will support broader data curation and KPI enhancement.
Figure: Title: IBD Pilot: Outcomes Analysis Caption: Table 1. Data in Action: Improved patient adherence using a novel IBD Dashboard. Results of a multi-site 6-month pilot.
Figure: Title: IBD Pilot: Attrition Patient Outcomes - Services Received Caption: Figure 1. Data in Action: Improved patient adherence using a novel IBD Dashboard. Results of a multi-site 6-month pilot.
Disclosures: Michael Mills indicated no relevant financial relationships. Gena Ettinger indicated no relevant financial relationships. Nicole Smith indicated no relevant financial relationships. Wanda Wilt: Cardinal Health – Employee. Paul Berggreen: Eli Lilly – Consultant. Specialty Networks – Stock Options.
Michael Mills, MD, MPH, FACG1, Gena Ettinger, PA-C, MSHS2, Nicole Smith, BS, MS3, Wanda L.. Wilt, 4, Paul Berggreen, MD5, 27, Data in Action: Improved Patient Adherence Using a Novel IBD Dashboard. Results of a Multi-Site 6-Month Pilot, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.



 photo")