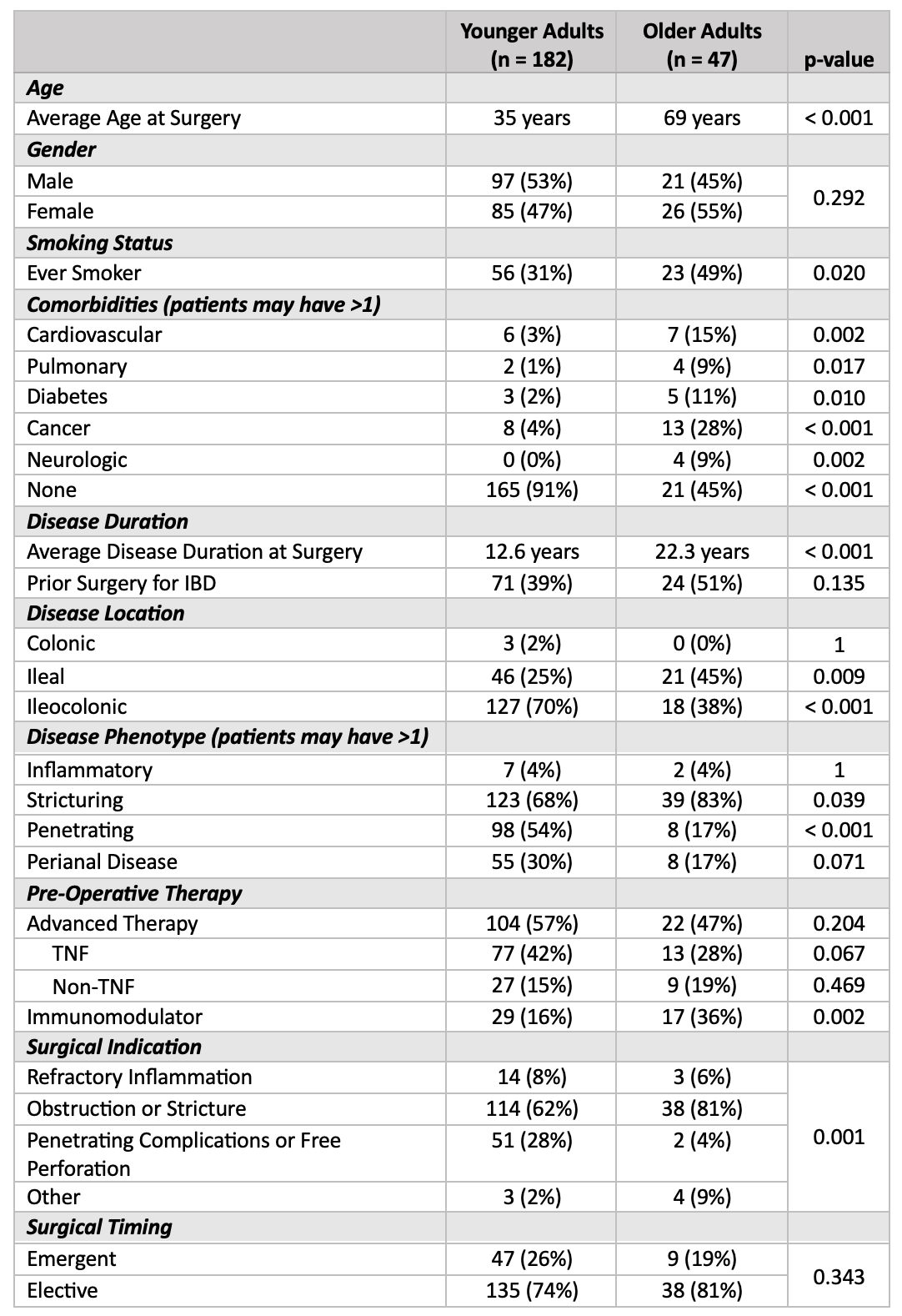
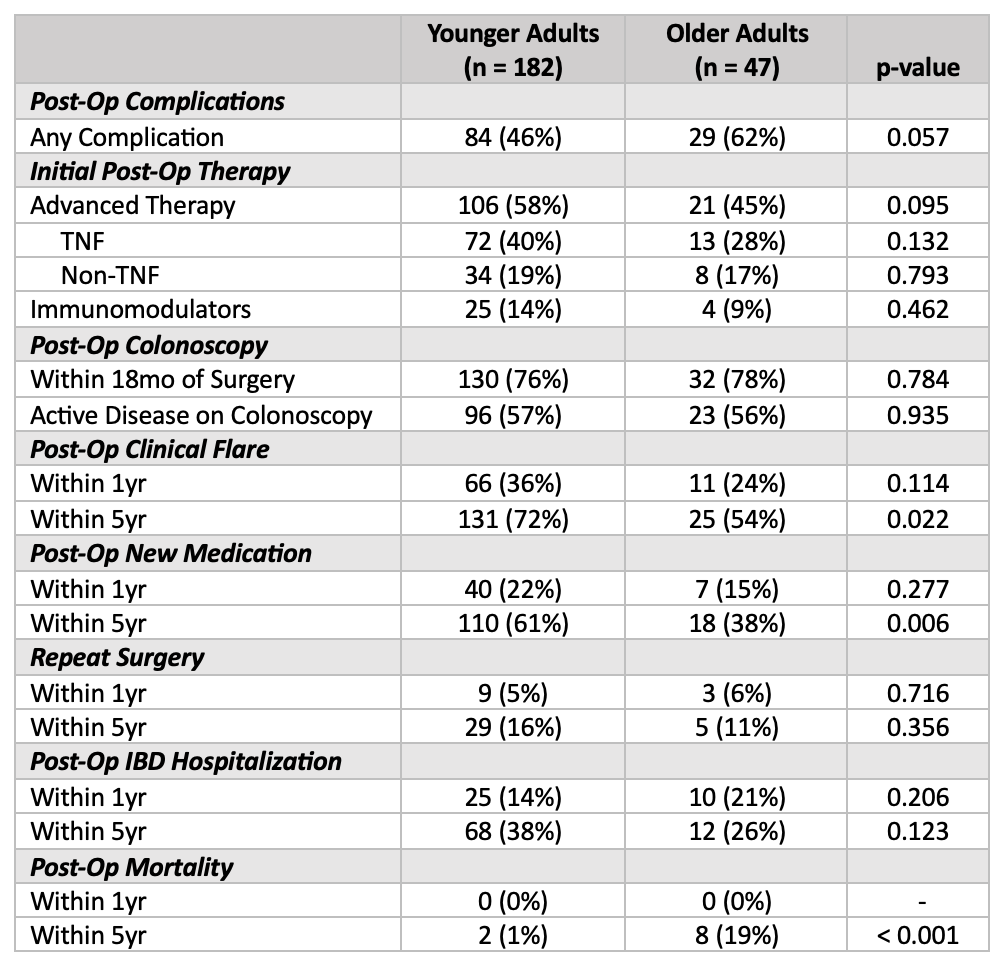
Hailey M. Harris, MD1, Sara Ghoneim, MD1, Bharati Kochar, MD1, Ashwin Ananthakrishnan, 2 1Massachusetts General Hospital, Boston, MA; 2Division of Gastroenterology, Massachusetts General Hospital and Harvard Medical School, Boston, MA Introduction: There is rising prevalence of Crohn’s disease (CD) among older adults. Nearly half of patients with CD require ileocecal resection. Contemporary post-operative management involves surveillance for recurrence and personalized approach to post-operative preventive therapy. The goal of this research was to investigate differences in management and outcomes following ileocecal resection in older adults with CD. Methods: We performed a retrospective cohort study of patients with CD who had undergone ileocecal resection with primary anastomosis between 2008-2023. We compared pre-operative characteristics and post-operative outcomes for patients age >60 years at time of index surgery versus younger patients. Primary study outcomes included post-operative complications, post-operative endoscopic surveillance, use of post-operative advanced therapy, clinical and surgical recurrence rates, and mortality. Multivariable models adjusting for confounders examined the impact of age on post-operative outcomes. Results: Our cohort included 47 older adults (age >60 years) and 182 younger patients (age 13-59 years). Older adults were more likely to have pre-operative comorbidities (55% vs. 9%, p< 0.001) and had longer disease duration at time of surgery (22.3yr vs. 12.6yr, p< 0.001). Older adults were also more likely to require surgery for stricturing complications (81% vs. 62%, p=0.001). There was a trend towards higher post-operative complication rates amongst older adults (62% vs. 46%, p=0.057). A similar fraction of older adults underwent colonoscopic surveillance within 18 months of surgery (78% vs. 76%, p=0.78) with similar rates of endoscopically active disease (56% vs. 57%, p=0.94). Older adults were similarly likely to initiate advanced therapy post-operatively compared to younger patients (45% vs. 58%, p=0.095). Within 5 years of surgery, older adults were significantly less likely to have a clinical flare (54% vs. 72%, p=0.022) or require transition to a different medication for CD (38% vs. 61%, p=0.006). However, older patients had a measurably higher 5-year mortality rate compared to younger patients (19% vs. 1%, p< 0.001). Discussion: Reassuringly, we found no significant difference in post-operative advanced therapy initiation or post-operative surveillance endoscopy between younger and older adults with CD. Older adults had similar short-term clinical and endoscopic recurrence rates with a milder long-term clinical course but overall higher mortality.
Figure: Table 1: Pre-operative patient demographics and operative comparisons
Figure: Table 2: Post-operative outcomes in younger and older patients
Hailey M. Harris, MD1, Sara Ghoneim, MD1, Bharati Kochar, MD1, Ashwin Ananthakrishnan, 2, 25, Differences in Outcomes Following Ileocecal Resection in Older Adults with Crohn’s Disease in the Biologic Era, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.



 photo")