Loma Linda University Medical Center Loma Linda, CA
Danyal Imam, MBBS, Nikhil Thiruvengadam, MD, Paul Leonor, MD, Kendrick Che, DO Loma Linda University Medical Center, Loma Linda, CA Introduction: Pancreatic Adenocarcinoma is a highly aggressive tumor with early local spread to adjacent organs as well as distant metastasis. We present a case of newly diagnosed pancreatic adenocarcinoma causing complete obstruction of the duodenum and creation of a false lumen.
Case Description/
Methods: A 62-year-old male with a history of Decompensated Cirrhosis and Type 2 Diabetes Mellitus initially presented to an outside hospital (OSH) with the complaint of abdominal pain. Magnetic Resonance Cholangiopancreatography (MRCP) demonstrated a cirrhotic liver with mild-moderate intrahepatic and extrahepatic biliary dilation, as well as numerous pancreatic cysts. Subsequent esophagogastroduodenoscopy (EGD) demonstrated a large mass in the duodenal bulb with necrotic mucosa. Tissue biopsy of the mass was notable for adenocarcinoma. He was then discharged with outpatient oncology follow up. However, the patient presented to OSH 5 days after discharge with worsening abdominal pain. A repeat MRCP demonstrated a large irregular multilobulated peri-pancreatic rim enhancing fluid collection containing multiple air-fluid levels. He was subsequently transferred to Loma Linda University Medical Center (LLUMC) for higher level of care. At LLUMC, the patient initially underwent Endoscopic Ultrasound for further evaluation where he was noted to have a 3.8 cm pancreatic head mass invading the duodenum resulting in duodenal obstruction. Tissue biopsies were taken with pathology consistent with adenocarcinoma of pancreatic ductal origin. The following day duodenal stent placement was attempted, however, after several attempts of guide-wire advancement and contrast injection, it was apparent that a large tumor cavity was in continuity with the duodenal bulb with no true lumen identified. The patient was later discharged home after successful diet advancement. Discussion: Pancreatic Cancer is the third leading cause of cancer related mortality. This is attributed to its aggressive nature resulting in rapid local spread as well as early distant metastasis. Surgical resection can be curative, however, only 20% of cases have surgically resectable disease at the time of diagnosis. Modifiable risk factors include smoking, obesity, and diabetes. There is currently no standardized method for pancreatic cancer screening. This case highlights, the importance of reducing modifiable risk factors for pancreatic cancer, particularly in the setting of limited screening modalities and presence of advanced disease on initial diagnosis.
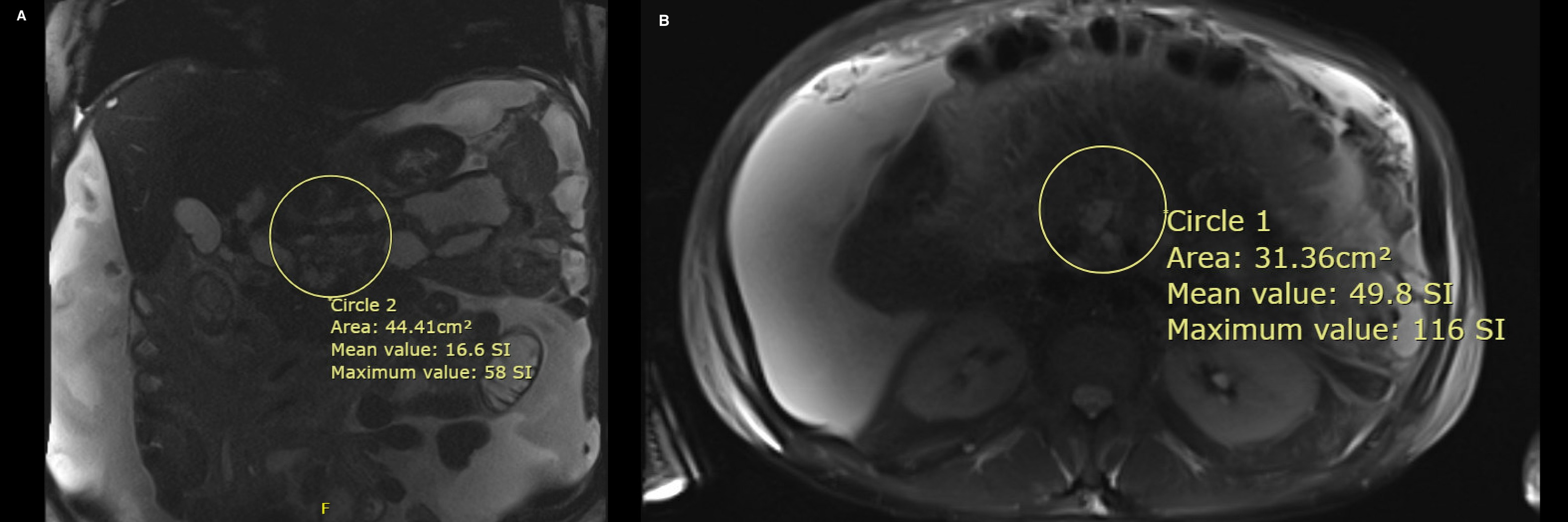
Figure: Ill-defined lesion centered at the pancreatic head with multiple large irregular pancreatic/peripancreatic rim-enhancing fluid collections with multiple air-fluid levels (Figure A and B)
Disclosures: Danyal Imam indicated no relevant financial relationships. Nikhil Thiruvengadam: Enterasense – Consultant. Paul Leonor indicated no relevant financial relationships. Kendrick Che indicated no relevant financial relationships.
Danyal Imam, MBBS, Nikhil Thiruvengadam, MD, Paul Leonor, MD, Kendrick Che, DO. P0140 - Lumen or Tumor Cavity? A Case of Invasive Pancreatic Cancer Creating a False Lumen, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.