Texas Tech University Health Sciences Center Lubbock, TX
Busara Songtanin, MD1, Grace McCrea, 1, Mackenzie Coffin, 1, Kanak Das, MD2, Tyler Mouw, MD1 1Texas Tech University Health Sciences Center, Lubbock, TX; 2Texas Tech University, Lubbock, TX Introduction: Pancreatic paraganglioma is a rare tumor and is usually benign. Here we present a case of pancreatic paraganglioma that was initially diagnosed with pancreatic neuroendocrine tumor.
Case Description/
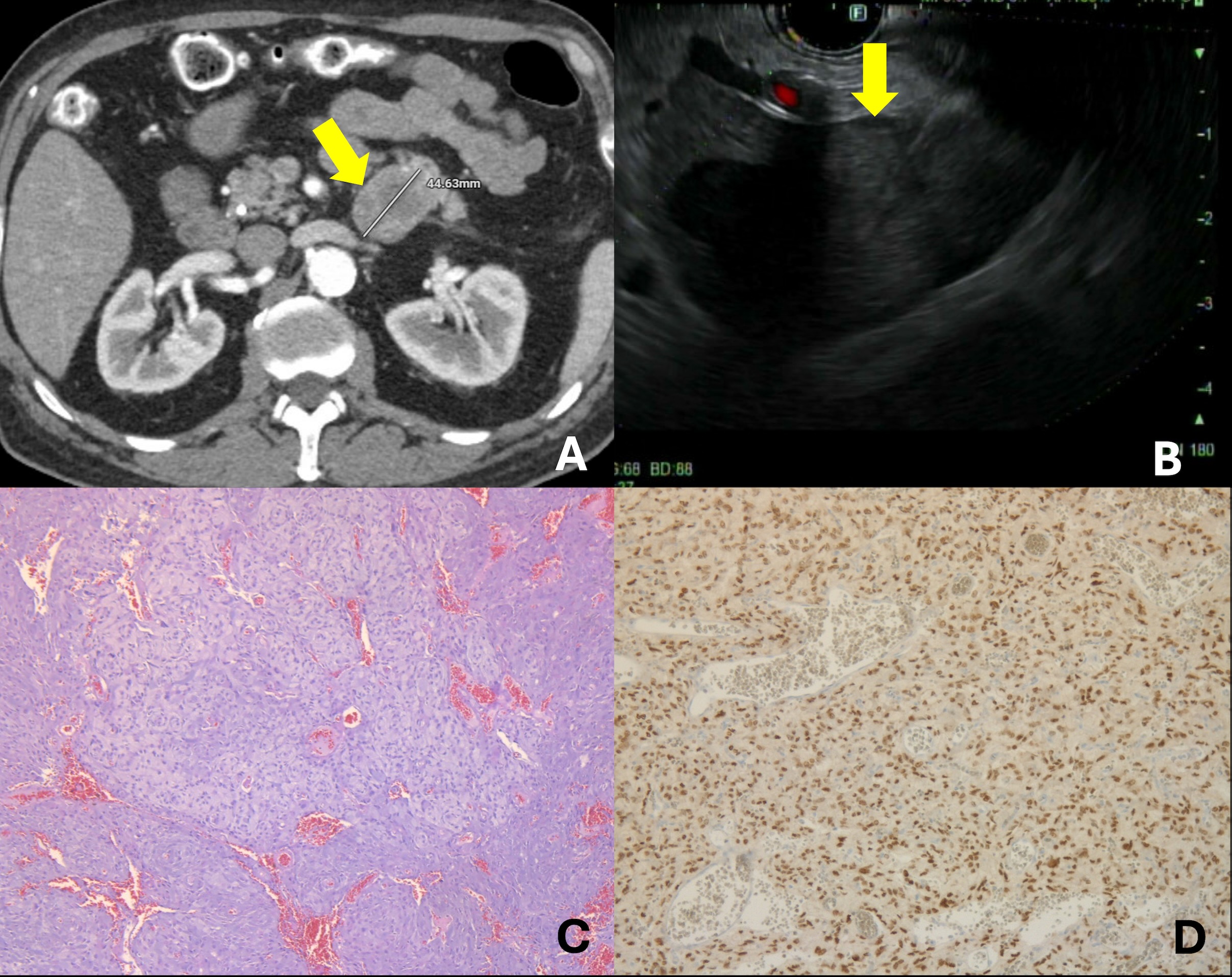
Methods: A 70-year-old man presented to the hospital with acute ascending cholangitis due to choledocholithiasis. A contrast-enhanced computed tomography of the abdomen incidentally revealed a 4.4 cm solid hypodense mass at the tail of the pancreas (Figure 1A). Endoscopic ultrasonography demonstrated a 47 mm x 40 mm hypoechoic, focally anechoic, solid, cystic, heterogeneous, irregular mass at the tail of the pancreas (Figure 1B). A fine needle biopsy of the mass was performed. Histopathology showed a well-differentiated neuroendocrine tumor. The patient underwent a distal pancreatectomy and splenectomy. Histopathology of the pancreatic mass with hematoxylin and eosin stain revealed epithelioid cells arranged in a trabecular pattern separated by a vascular network (zellballen pattern). The immunohistochemical staining showed strong nuclear reactivity for GATA3 and loss of expression of SDHB, supporting the diagnosis of pancreatic paraganglioma. There was no lymphovascular invasion. At 6-month follow-up, the patient remained symptom-free without evidence of distant metastasis on a contrast-enhanced computed tomography of the chest, abdomen, and pelvis. Discussion: The paraganglia are clusters of neuroendocrine cells consisting of both sympathetic and parasympathetic nervous systems. Pancreatic paragangliomas are extremely rare. They are usually benign and non-functional. In functional tumors, symptoms may mimic pheochromocytoma due to high levels of catecholamine. The disease is often indistinguishable from pancreatic neuroendocrine tumor preoperatively. In this case, despite extensive imaging and biopsy, the diagnosis was confirmed postoperatively. This case highlights the limitations of current diagnostic modalities and the importance of using the immunohistochemical stain in distinguishing between pancreatic neuroendocrine tumors and paragangliomas. Surgical removal of the tumor is the definitive treatment for pancreatic paraganglioma. Additionally, the preoperative diagnosis of paragangliomas is crucial for surgical planning due to the need for alpha-blockade medications to prevent intraoperative hemodynamic instability. Recognition of this rare neoplasm is also important for appropriate genetic counseling and postoperative management.
Figure: (A)The computed tomography pancreatic protocol revealed a 4.4 cm solid mass located dorsal to the tail of the pancreas (yellow arrow). (B)Endoscopic ultrasound showed a 47 mm x 40 mm hypoechoic and focally anechoic solid cystic heterogeneous, irregular mass at the tail of the pancreas (yellow arrow). (C)Pathology with hematoxylin and eosin stain showed round oval cells arranged in organoid and trabecular patterns separated by a delicate vascular network (zellballen pattern) (D)Pathology showed diffuse strong nuclear reactivity for GATA 3 in chief cells.
Disclosures: Busara Songtanin indicated no relevant financial relationships. Grace McCrea indicated no relevant financial relationships. Mackenzie Coffin indicated no relevant financial relationships. Kanak Das indicated no relevant financial relationships. Tyler Mouw indicated no relevant financial relationships.
Busara Songtanin, MD1, Grace McCrea, 1, Mackenzie Coffin, 1, Kanak Das, MD2, Tyler Mouw, MD1. P0134 - Pancreatic Paraganglioma: A Rare Tumor With Diagnostic Challenges, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.