Long Island Jewish Forest Hills Hospital - Northwell Health Queens, NY
WonKyung Cho, MD, MPH1, Ken Chan, DO2, Olawole Olafisoye, MD2 1Long Island Jewish Forest Hills Hospital - Northwell Health, Queens, NY; 2Long Island Jewish Forest Hills Hospital - Northwell Health, Forest Hills, NY Introduction: Vasculitis involving mesenteric vessels is rare and typically occurs as part of systemic disease. Isolated superior mesenteric artery (SMA) vasculitis is an uncommon entity that may present with vague gastrointestinal symptoms and, if unrecognized, can lead to significant morbidity. We report a rare case of isolated SMA vasculitis in the absence of systemic involvement.
Case Description/
Methods: A 57-year-old male with past medical history of hypothyroidism, paroxysmal atrial fibrillation and hypertension presented with a 5-day history of abdominal pain. The pain began suddenly, was initially diffuse, but became sharp and localized to the epigastric area, radiating to the back. The pain was constant and unrelated to eating. He denied fevers, diarrhea, gastrointestinal bleeding, or joint symptoms. Physical exam was notable for mild epigastric tenderness without peritoneal signs. On exam, mild epigastric tenderness was noted without peritoneal signs. Laboratory results showed normal complete blood count and liver enzymes. C-reactive protein (20.1mg/L) was elevated but erythrocyte sediment rate (18 mm/hr) was within normal limits. Although complement levels (C3 164 mg/dl, C4 40 mg/dl) were in the upper normal, other autoimmune serologies, including antinuclear antibodies (ANA), antineutrophil cytoplasmic antibodies (ANCA), double stranded DNA (dsDNA), and hepatitis pane were unremarkable. Computed tomography (CT) angiography revealed severe proximal SMA stenosis with surrounding inflammatory fat stranding and a 1.4 x 0.7 cm aneurysmal dilation, suggestive of vasculitis. No signs of bowel edema or ischemia were present. Given the absence of systemic disease and ischemic complications, surgical intervention was deferred. The patient was started on oral prednisone 1 mg/kg daily, resulting in marked clinical improvement. Discussion: Isolated SMA vasculitis is a rare and potentially under-recognized cause of mesenteric ischemia. Diagnosis can be challenging due to nonspecific symptoms and often normal serologies. Imaging, particularly CTA, is crucial for identifying vascular inflammation as biopsy is rarely feasible due to anatomical constraints. This case adds to limited existing literature, highlighting the importance of recognizing isolated SMA vasculitis even in the absence of systemic features. Early diagnosis and timely initiation of immunosuppressive therapy can prevent progression to intestinal ischemia and improve patient outcomes.
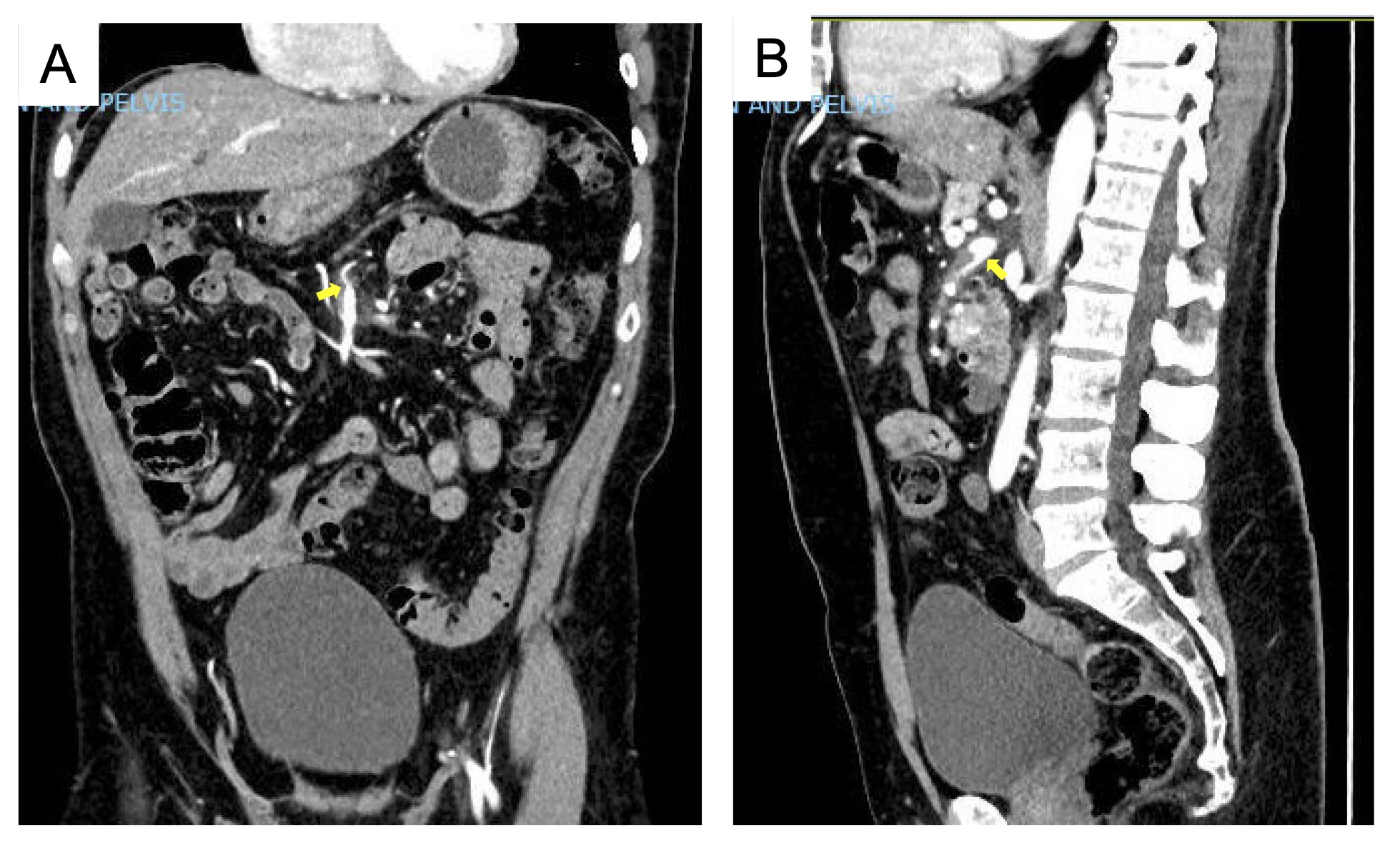
Figure: Figure. CT Abdomen showing (A) severe proximal SMA stenosis with surrounding inflammatory fat stranding, suggestive of vasculitis, (B) a focal outpouching along the course of the SMA superiorly measuring 1.4 cm x 0.7 cm.
Disclosures: WonKyung Cho indicated no relevant financial relationships. Ken Chan indicated no relevant financial relationships. Olawole Olafisoye indicated no relevant financial relationships.
WonKyung Cho, MD, MPH1, Ken Chan, DO2, Olawole Olafisoye, MD2. P0363 - A Burning Branch: Isolated Superior Mesenteric Artery Vasculitis as a Rare Cause of Abdominal Pain, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.