Award: ACG Outstanding Research Award in the Colorectal Cancer Prevention Category (Trainee)
Award: ACG Presidential Poster Award
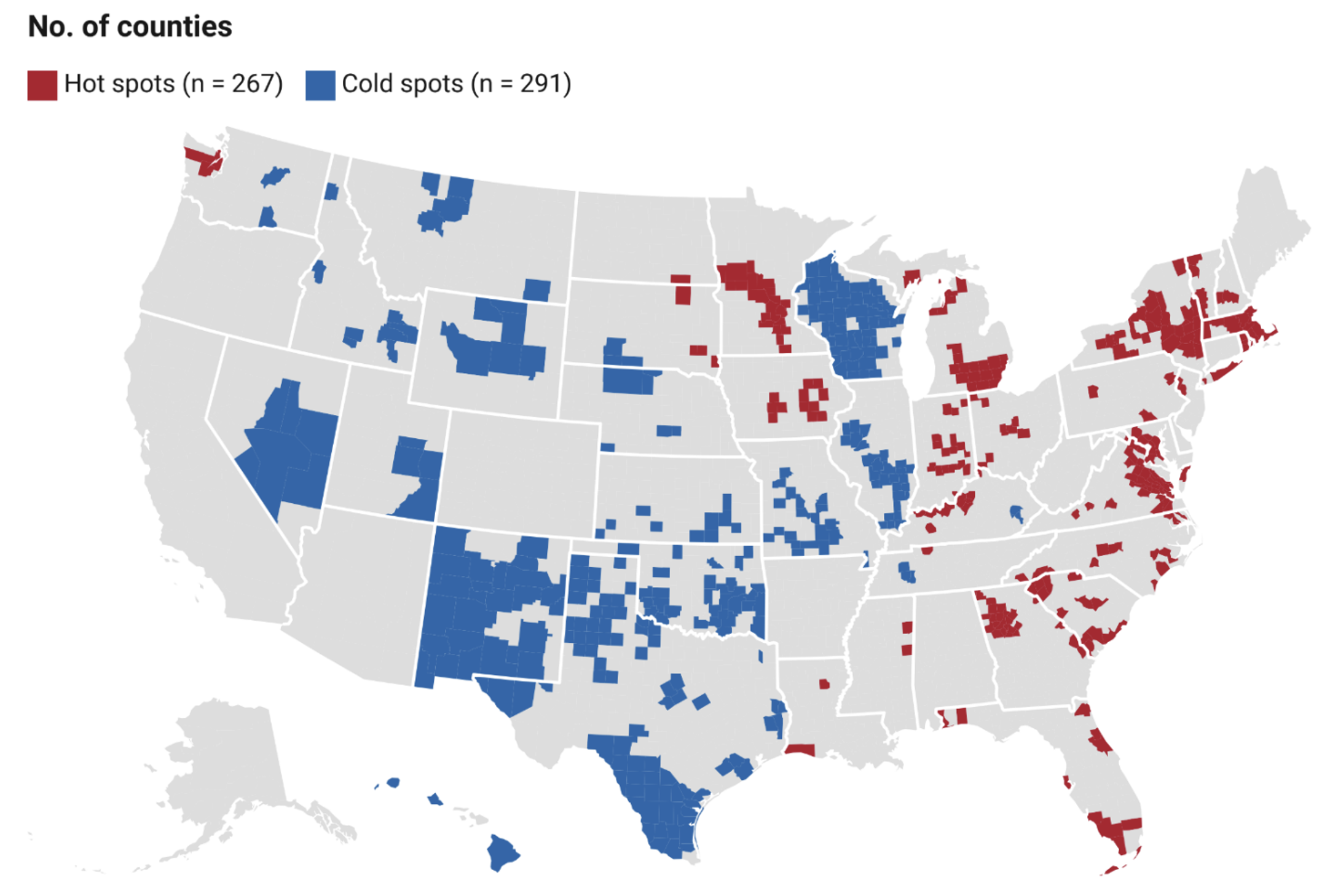
Ahmed Al Qady, MD1, Wafa Aldhaleei, MD2, Akshaya Bhagavathula, PhD3 1University of Florida, Gainesville, FL; 2Mayo Clinic, Rochester, MN; 3North Dakota State University, Fargo, ND Introduction: Colorectal cancer (CRC) screening has been proven to reduce mortality, but the COVID-19 pandemic disrupted preventive care nationwide. Geospatial analysis offers a powerful lens to examine local changes in screening and identify care differences. We conducted a nationwide county-level analysis to assess shifts in CRC screening from 2018 to 2023 and evaluated how social vulnerability influenced these trends. Methods: We used model-based, age-adjusted CRC screening prevalence estimates from the CDC PLACES Project for adults aged 50–75 years, comparing the pre-pandemic (2018–2019) and post-pandemic (2022–2023) periods. We applied Local Moran’s I to identify spatial clusters of change (ΔRate) and classified counties as high–high (hotspot), low–low (coldspot), high–low, or low–high. We stratified clusters by 2022 Social Vulnerability Index (SVI) and state. Results: Among 3,108 U.S. counties, the median change in CRC screening prevalence between the pre and post pandemic periods was +1.6 percentage points (interquartile range [IRQ]: –2.3 to +5.2). A total of 240 counties (7.7%) were identified as hotspots and 291 counties (9.4%) as coldspots. (Figure 1) Hotspots were primarily located in the Southeast and Mid-Atlantic regions, especially in Virginia (n=40), New York (n=27), and Georgia (n=24). Coldspots were concentrated in the Midwest and South-Central U.S., particularly in Texas (n=78), Wisconsin (n=51), and Oklahoma (n=31).
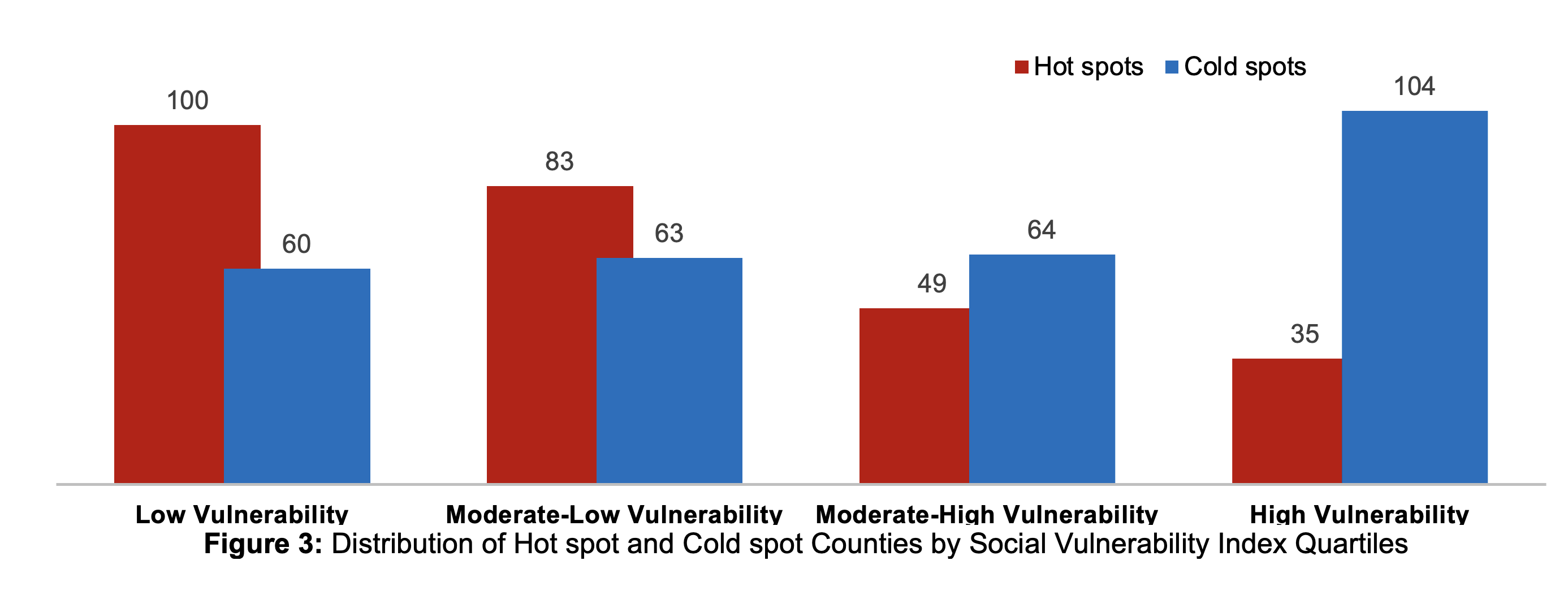
When stratified by social vulnerability, 41.7% of hotspot counties were in the least vulnerable quartile (SVI Q1), while 35.7% of coldspots were in the most vulnerable quartile (SVI Q4). (Figure 2) Discussion: This is the first nationwide study to use geospatial analysis to assess changes in CRC screening following the COVID-19 pandemic. We found an uneven recovery, with hotspots concentrated in less socially vulnerable counties, and coldspots clustering in more vulnerable areas.
Unlike prior studies that offer cross-sectional snapshots, our analysis captures changes over time, providing a dynamic view of how screening utilization evolved during the recovery period. This temporal perspective identifies not just where care gaps exist, but how they have shifted, offering actionable insights to close screening gaps and improve population-level cancer prevention. While ecological in nature, these findings can guide resource allocation and inform future research into the drivers of resilience and vulnerability in CRC screening.
Figure: Figure 1
Figure: Figure 2
Disclosures: Ahmed Al Qady indicated no relevant financial relationships. Wafa Aldhaleei indicated no relevant financial relationships. Akshaya Bhagavathula indicated no relevant financial relationships.
Ahmed Al Qady, MD1, Wafa Aldhaleei, MD2, Akshaya Bhagavathula, PhD3. P0526 - Examining Colorectal Cancer Screening Patterns Across US Counties Using Geospatial Analysis Pre- and Post-COVID-19, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.