Muhammad Umer Mukhtar, MD, Fatima Warraich, MD, Erik Olson, DO Rochester General Hospital, Rochester, NY Introduction: The right subclavian artery typically arises from the aortic arch, however in 0.5%–2% of individuals, an aberrant right subclavian artery (ARSA) originates from the proximal descending aorta, coursing anterior or posterior to the esophagus or trachea. Aneurysmal dilation, seen in approximately 60% of cases, is known as Kommerell diverticulum. Compression of the aerodigestive tract may cause dysphagia (termed dysphagia lusoria), cough, stridor, chest pain, or upper limb ischemia.
Case Description/
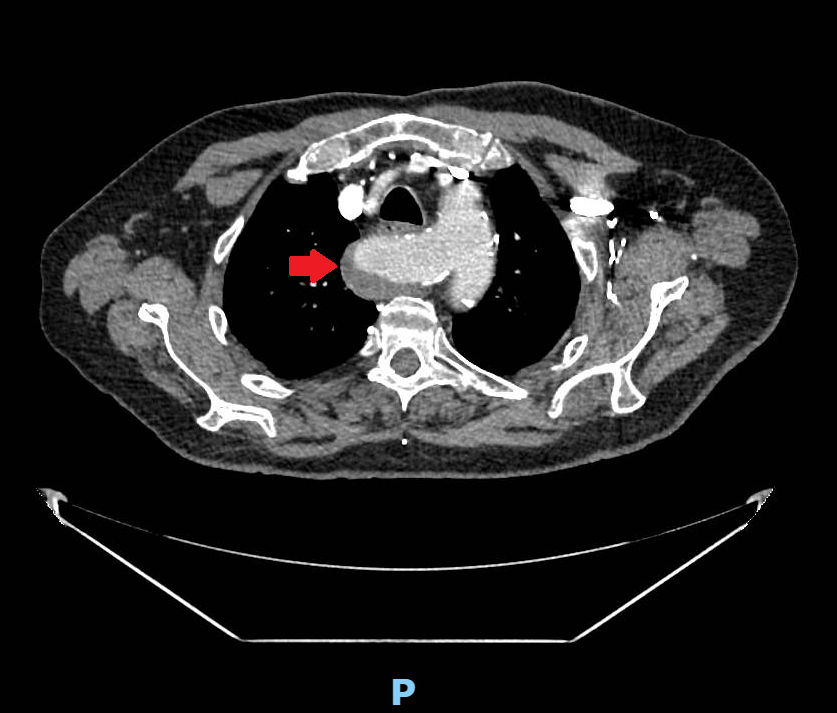
Methods: An 82-year-old man with a medical history of hypertension, hyperlipidemia presented after a fall. A chest X-ray revealed an incidental bilateral paratracheal prominence. Subsequent CT angiography demonstrated an aberrant right subclavian artery with a retroesophageal course and a 3.6 cm aneurysmal dilation at its origin with mural thrombus (Figure 1) - findings consistent with Kommerell diverticulum. Vascular surgery was consulted and due to the size of the aneurysm, surgical repair was recommended.
The patient underwent right carotid-to-subclavian bypass, ligation of the aberrant subclavian artery, and placement of thoracic branch endograft to exclude the aneurysm. On post-operative day 1, he experienced dysphagia to liquids, which resolved after a 3 day course of prednisone (10 mg daily). At his two-week follow-up, CTA confirmed successful repair. However, three weeks post-operatively, he returned with progressive dysphagia to solids and liquids for three days. Repeat CT angiography demonstrated esophageal compression from the repaired Kommerell diverticulum. A short course of methylprednisolone led to resolution of his symptoms. At his three-month gastroenterology follow-up, he remained asymptomatic. Discussion: CT angiography is the preferred imaging modality for evaluating Kommerell diverticulum. Surgical repair, either open or endovascular, is indicated for symptomatic cases or asymptomatic cases with a diameter greater than 3 cm. As illustrated by this case, dysphagia may present both pre- or post-operatively. In our case, steroids were used empirically to manage presumed post-surgical inflammation with resolution of symptoms.
Figure: Figure 1: Kommerel diverticulum with associated mural thrombus
Disclosures: Muhammad Umer Mukhtar indicated no relevant financial relationships. Fatima Warraich indicated no relevant financial relationships. Erik Olson indicated no relevant financial relationships.
Muhammad Umer Mukhtar, MD, Fatima Warraich, MD, Erik Olson, DO. P0769 - Kommerell Diverticulum: A Unique Etiology of Dysphagia, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.