Dharma Ayer, BS1, Caesar Ferrari, BS1, Kumael Jafri, BS1, Sonia Samuel, DO1, Dana Gornick, MD2, Paul Feustel, MEng, PhD1, Micheal Tadros, MD1 1Albany Medical Center, Albany, NY; 2Cedars-Sinai Medical Center, Los Angeles, CA Introduction: Esophagogastroduodenoscopy (EGD) is a key diagnostic tool for upper gastrointestinal (GI) disorders, yet quality indicators are less standardized compared to colonoscopy. Recent studies suggest that procedural time may correlate with diagnostic yield. However, time is not currently a recognized quality benchmark. This study evaluates the relationship between EGD duration and the detection of clinically significant findings (CSFs), while examining procedural parameters. Methods: We retrospectively analyzed 120 first-time diagnostic EGDs performed at a single academic center. Procedures were grouped by duration: < 3 minutes, 3 to 6 minutes, and >6 minutes. The relationship between procedure time and CSF detection were evaluated using chi-square and Cochran-Armitage trend tests. Univariable and multivariable logistic regression models were used to identify independent predictors of CSF detection, including procedural time, clinical indication, and procedural metrics (photographs, biopsies, landmarks). Secondary analyses evaluating the relationship between procedural duration and other metrics were conducted using ANOVA and linear regression. Results: EGD duration was significantly associated with a stepwise increase CSF detection. Compared to procedures < 3 minutes, those lasting > 6 minutes had 17.5-fold increased odds of identifying a CSF (p = 0.016). The “bleeding” (OR 10.0, p = 0.022) and “other” indication categories (OR 8.42, p = 0.033) were also independently predictive of higher CSF detection. While increased photographs and landmark identification correlated with longer duration, neither independently predicted CSFs in adjusted models. Time being 3 to 6 and > 6 minutes showed stepwise increases in photographs (p < 0.001), landmark identification (p < 0.001), and biopsies (p < 0.05), supporting time as a variable that integrates multiple quality metrics. Discussion: Procedure duration may serve as a standardized quality metric for diagnostic upper endoscopy, independently associated with increased detection of CSFs in a stepwise manner. In addition, it may function as a unifying measure correlated with multiple quality metrics indicative of comprehensiveness in performing the EGD. Incorporating minimum time thresholds into routine diagnostic EGDs for first-time procedures and particularly in high-yield indications like bleeding, may enhance diagnostic performance and complement existing quality frameworks.
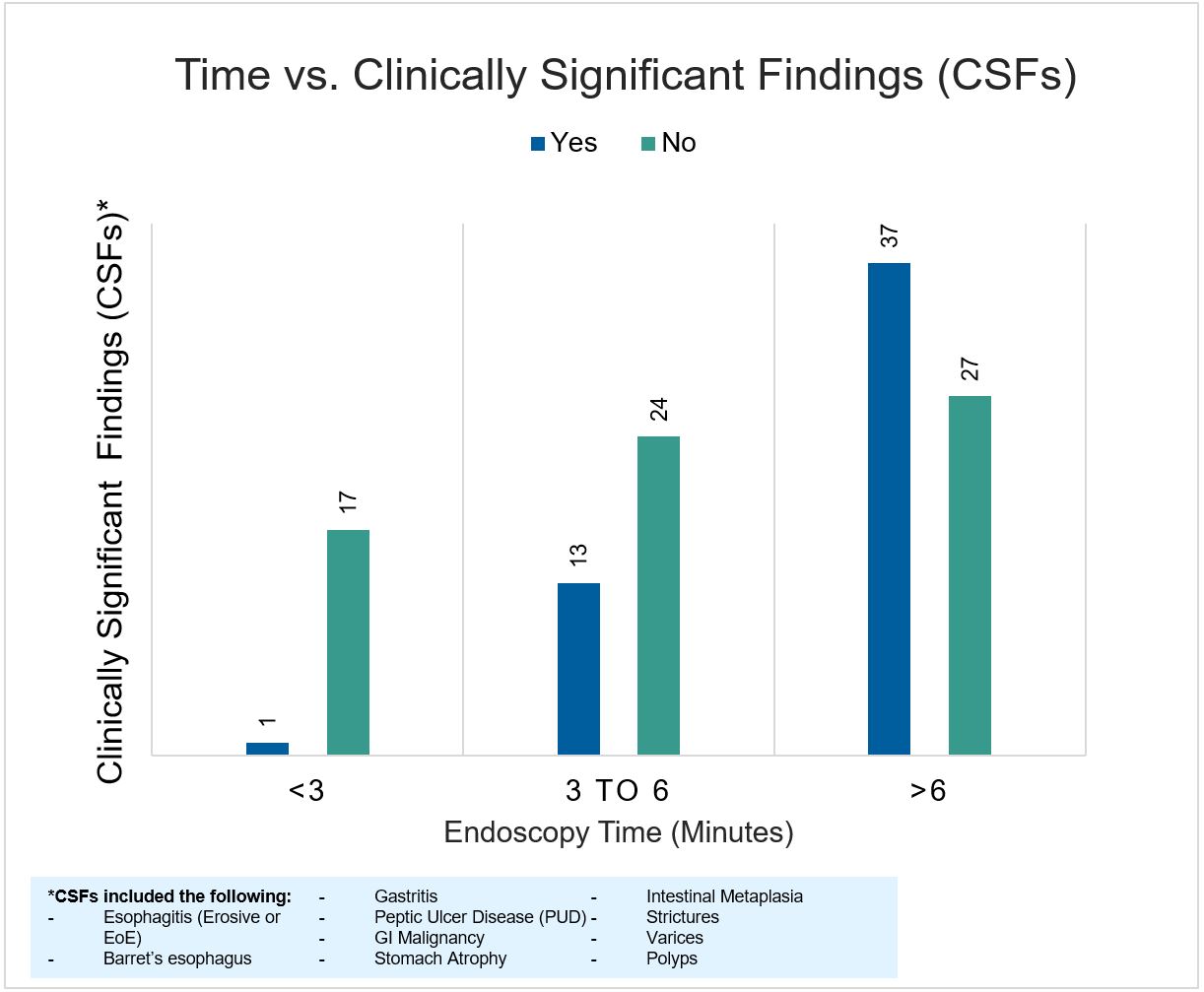
Figure: Figure 1: Distribution of clinically significant findings (CSFs) by endoscopy duration category. CSFs were more frequently identified in procedures lasting longer than 3 minutes, with the highest detection rate observed in those exceeding 6 minutes.
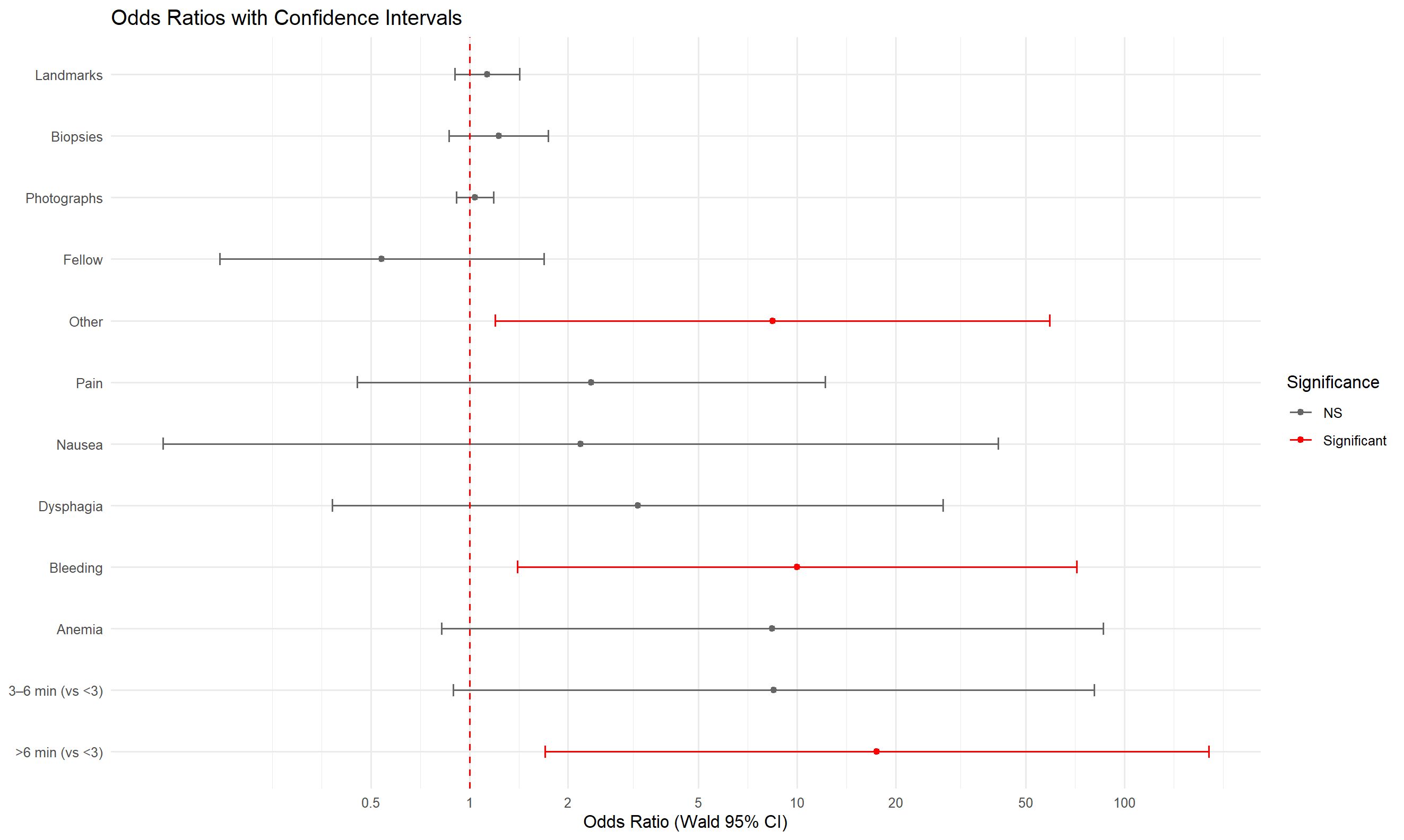
Figure: Figure 2: Multivariable logistic regression model showing odds ratios (ORs) and 95% confidence intervals (CIs) for predictors of clinically significant findings (CSFs) during EGD. Significant predictors are shown in red and include procedure duration > 6 minutes, bleeding, and “other” clinical indications. All other variables, including number of photographs, biopsies, landmarks identified, and operator type, did not reach statistical significance.
Disclosures: Dharma Ayer indicated no relevant financial relationships. Caesar Ferrari indicated no relevant financial relationships. Kumael Jafri indicated no relevant financial relationships. Sonia Samuel indicated no relevant financial relationships. Dana Gornick indicated no relevant financial relationships. Paul Feustel indicated no relevant financial relationships. Micheal Tadros indicated no relevant financial relationships.
Dharma Ayer, BS1, Caesar Ferrari, BS1, Kumael Jafri, BS1, Sonia Samuel, DO1, Dana Gornick, MD2, Paul Feustel, MEng, PhD1, Micheal Tadros, MD1. P0842 - Relationship Between EGD Duration and Clinically Significant Findings (CSFs): Time as a Quality Indicator of Upper Endoscopy, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.


 photo")