P0913 - Decreased 90-Day Mortality Seen With Resumption of Anticoagulation and Performance of Endoscopic Procedures in Patients Hospitalized With a GI Bleed
Osama Kaddourah, MD, MPH1, Qamar Iqbal, MD1, Christina Gomez, MD2, Huzaifa Khalid, MD1, Umme Ferdaush, MD1 1TidalHealth Peninsula Regional, Salisbury, MD; 2Saint Luke's Health System of Kansas City, Kansas City, MO Introduction: The evidence supporting post-endoscopic management of anticoagulation after bleeding is lacking consensus. Many studies favor resumption of agents to mitigate thrombotic risks; however, timing of resumption is also debatable. Methods: Non-interventional prospective study of all patients in our hospital who were admitted for GI bleeding while on anticoagulation in 2022. The primary outcomes were GI bleeding events, thrombotic events and mortality events within 90 days. We ran a logistic regression analysis to assess correlation between resumption of anticoagulation and primary outcomes. We ran a Mantel-Haenszel analysis between primary outcomes, various bleeding scores to determine a safe timing of resumption in our patient population. Results: 140 patients met our inclusion criteria. Resumption of anticoagulation was significantly associated with decrease in mortality events (p-value 0.001, CI 95% (-0.4 - -0.174)) while there was no association with bleeding or thrombotic events. Performing an endoscopic evaluation was associated with decrease in mortality events events (P value 0.025, CI 95% -0.282 - -0.019) and no association with bleeding or thrombotic events. As for timing, there was no significant difference in mortality, bleeding or thrombotic events between days of anticoagulation restart. We assessed timing of anticoagulation resumption based on CHADsVASc, HAS-BLED, Oakland, Glascow Blatchford score. We found these scores did not predict adverse events except a high HAS-BLED score predicted bleeding if resumption was on day 0 of admission. Discussion: Resumption of anticoagulation seems to be safe and should be prompt once bleeding is addressed. Performance of endoscopic procedures was associated with decreased mortality even in high-risk patients. Decision and safety of anticoagulation seem to be more dependent on the overall status of the patients after their bleeding events are addressed rather than how it was addressed or how they presented.
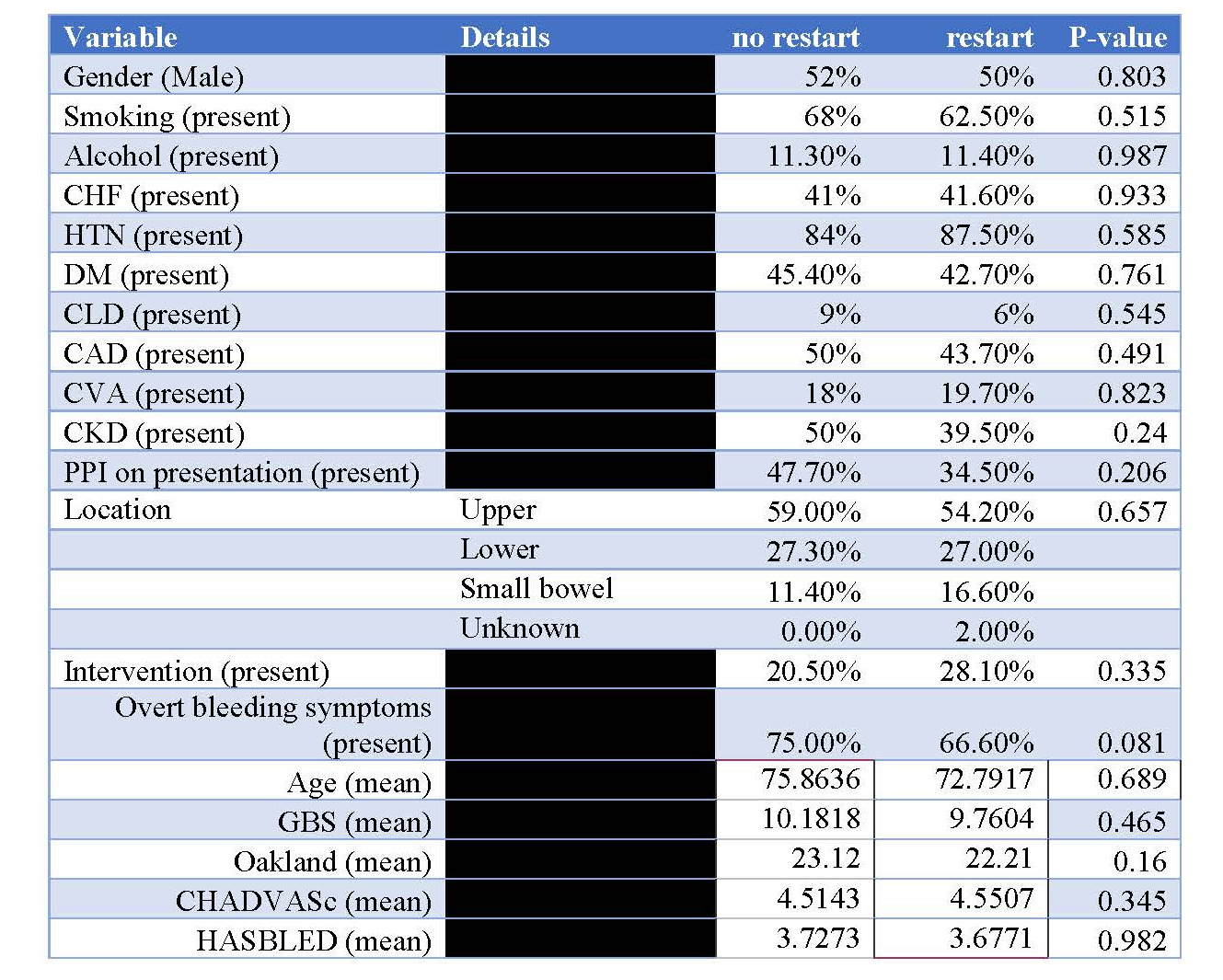
Figure: Table (1): Comparison of different variables collected between two groups of patients based on resumption of anticoagulation and their P-values. CHF: congestive heart failure, HTN: hypertension, DM: diabetes mellitus, CLD: chronic liver disease, CAD: coronary artery disease, CVA: cerebrovascular accident, CKD: chronic kidney disease, AC: anticoagulation, PPI: proton pump inhibitor, GBS: Glascow Blatchford score
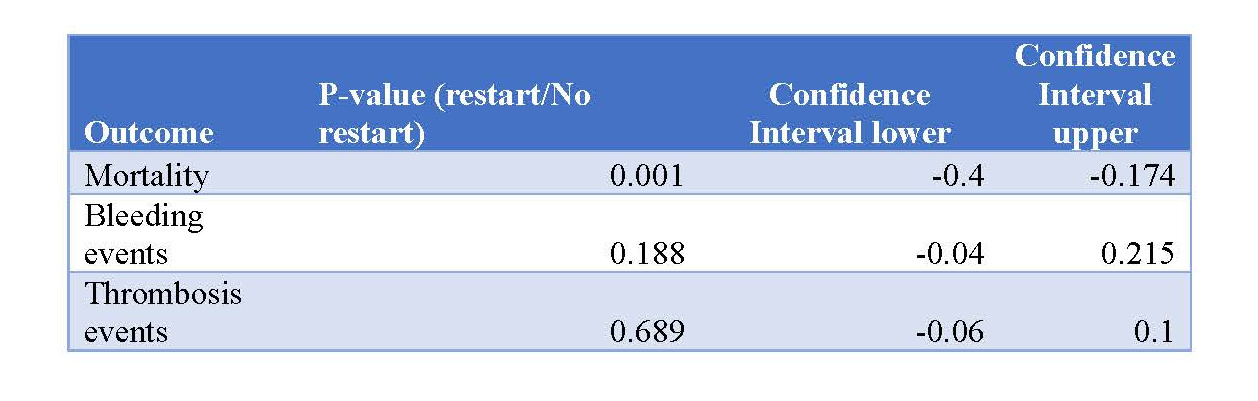
Figure: Table (2): Correlation between resumption of anticoagulation and our three primary outcomes.
Disclosures: Osama Kaddourah indicated no relevant financial relationships. Qamar Iqbal indicated no relevant financial relationships. Christina Gomez indicated no relevant financial relationships. Huzaifa Khalid indicated no relevant financial relationships. Umme Ferdaush indicated no relevant financial relationships.
Osama Kaddourah, MD, MPH1, Qamar Iqbal, MD1, Christina Gomez, MD2, Huzaifa Khalid, MD1, Umme Ferdaush, MD1. P0913 - Decreased 90-Day Mortality Seen With Resumption of Anticoagulation and Performance of Endoscopic Procedures in Patients Hospitalized With a GI Bleed, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.