Jeremy Zimmerman, MD, Robert J. Sealock, MD, Jordan Sparkman, MD, Gabriel Sandoval, MD Baylor College of Medicine, Houston, TX Introduction: Plasmablastic lymphoma (PBL) is an aggressive disease that commonly presents as an oral lesion in patients with human immunodeficiency virus (HIV). The vast differential for malignancies in this population makes endoscopy with tissue biopsy a critical step to establishing its diagnostic immunophenotype. Herein, we present a complex case of primary anorectal PBL in an HIV-positive patient with a history of rectal adenocarcinoma.
Case Description/
Methods: A 67-year-old male with a history of controlled HIV and stage IIIc rectal adenocarcinoma status post chemoradiation with tumor response, on maintenance pembrolizumab, presented 6 months after diagnosis with lower gastrointestinal bleeding. Initial colonoscopy revealed a 4-cm ulcerating rectal mass that extended into the anal canal. Biopsies were negative for malignancy. Repeat endoscopy at 4 and 8 month intervals showed rectal stricture and fibrosis, but biopsies remained negative for malignancy.
Approximately 1-year later, surveillance CT imaging revealed a new mass in the posterolateral wall of the rectum with an enlarged mesenteric lymph node. Ultimately, repeat flexible sigmoidoscopy with biopsy of ulcers in the rectum and anus revealed plasmablastic lymphoma without evidence of known rectal adenocarcinoma. Additional tissue biopsy of a retroperitoneal lymph node corroborated a new lymphoma diagnosis. Discussion: PBL is a rare subtype of diffuse large B-cell lymphoma associated with immunodeficiency such as HIV infection. It comprises 2.6% of all HIV-associated non-Hodgkin’s lymphoma diagnoses and has a significant male predominance. PBL typically manifests as a mass or ulcer inside the oral cavity. The mechanism for PBL’s oral predilection is not understood and a primary anorectal lesion is rarely described in the literature. PBL has also been rarely described to occur in the esophagus, stomach, and small intestine. On histology, PBL’s immunophenotype is characterized by expression of plasma cell markers with the absence of B-cell markers. Previous reports have identified up to 72% of PBLs are Epstein-Barr virus (EBV) positive, suggesting EBV infection may have a role in PBLs pathogenesis, although EBV-related mutations are less common in extra-oral disease. Historically, PBL portends a poor prognosis, high relapse rates, and median overall survival of less than 2 years, despite intense therapy. This case highlights a rare, but clinically important cause of anorectal malignancy in immunodeficient patients, such as those with HIV.
Figure: Surveillance CT revealing a new 4.5 cm heterogenously enhancing mass in the left posterolateral wall of the lower rectum/anus
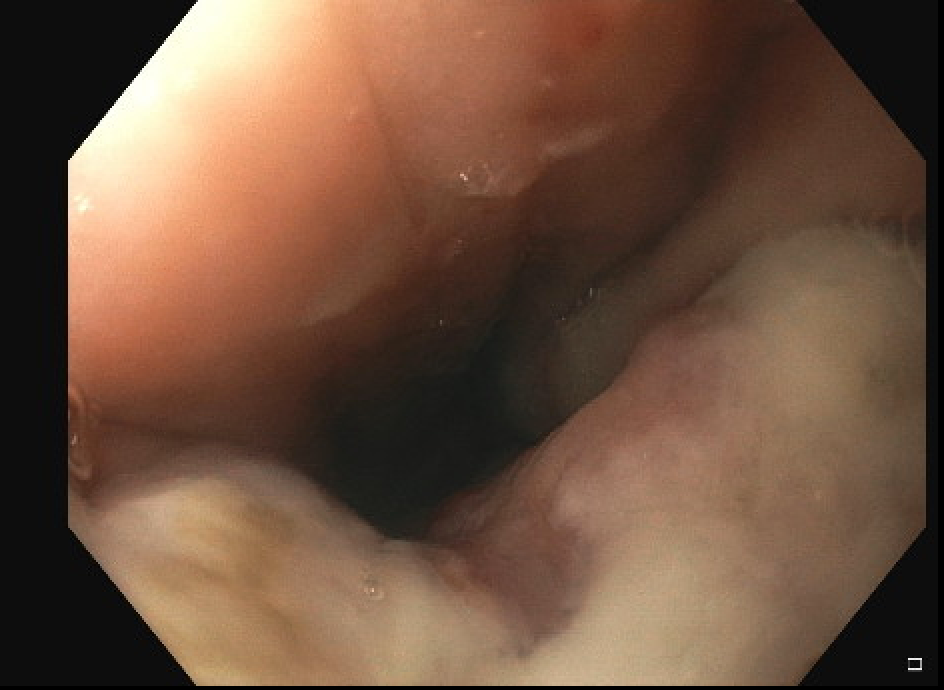
Figure: Endoscopic image of fibrotic and broadly ulcerated tissue extending distally into the anal canal
Disclosures: Jeremy Zimmerman indicated no relevant financial relationships. Robert Sealock indicated no relevant financial relationships. Jordan Sparkman indicated no relevant financial relationships. Gabriel Sandoval indicated no relevant financial relationships.
Jeremy Zimmerman, MD, Robert J. Sealock, MD, Jordan Sparkman, MD, Gabriel Sandoval, MD. P0979 - A Case of Primary Anorectal Plasmablastic Lymphoma, a Rare and Unexpected Endoscopy Finding in a Patient With HIV and Rectal Adenocarcinoma, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.