St. Luke's University Health Network Bethlehem, PA
Shivani K. Desai, MD1, Berhanu Geme, MD2 1St. Luke's University Health Network, Bethlehem, PA; 2St Luke’s University Health Network, Center Valley, PA Introduction: Duodenal diverticular bleeding is an extremely rare complication which may occur in older or middle-aged adults. Duodenal diverticula occur in 2 to 5% of patients [1]. They usually are of little significance; however, they can lead to complications such as obstruction and hemorrhage. Diagnosis is typically made by upper endoscopy or CT imaging.
Case Description/
Methods: A 71-year-old female with a past medical history of CVA on clopidogrel and aspirin, type 2 diabetes, estrogen receptor positive right sided breast cancer s/p mastectomy on chemotherapy and radiation, urinary incontinence, hyperlipidemia presented to the hospital with dizziness, nausea, and hematemesis along with hematochezia. Patient had a near syncopal witnessed event.
Patient endorsed having worsening fatigue and was noted to have 2 episodes of large bloody bowel movement once in the hospital. Hemoglobin on admission found to be 7 g/dL down from a baseline of 12 g/dL. Patient was also noted to be tachycardic and hypotensive
High volume CT imaging obtained of abdomen and pelvis in the emergency department was notable for an active bleed just distal to gastroduodenal junction involving the proximal duodenum/D1 segment with an adjacent diverticulum.
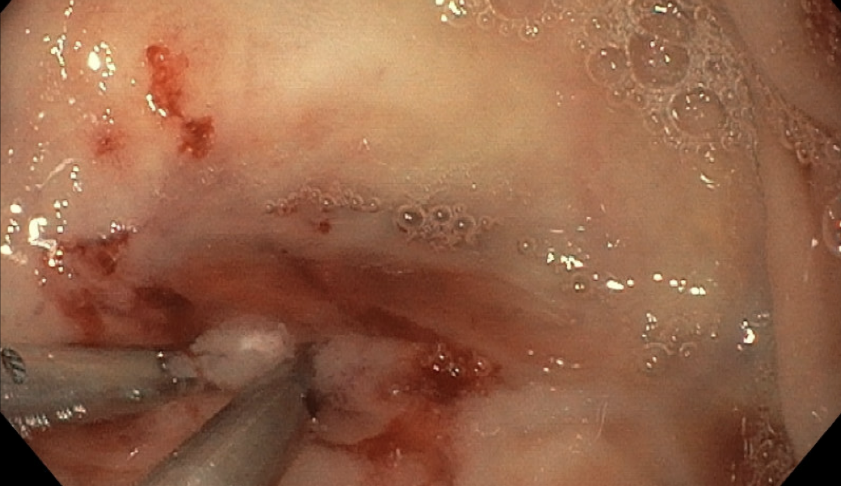
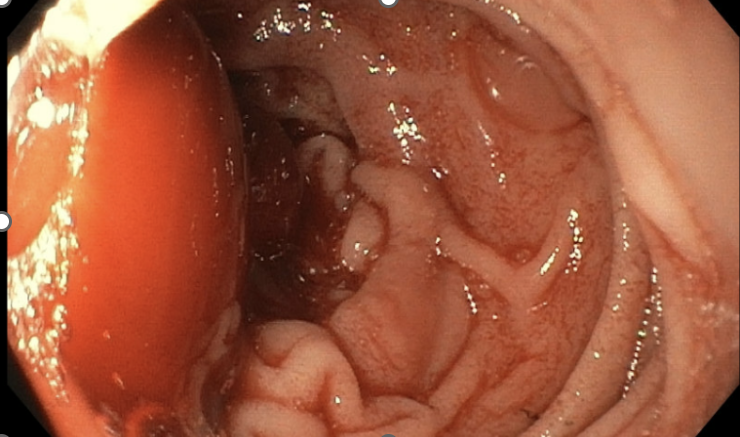
Patient underwent an emergent Esophagogastroduodenoscopy (EGD). The procedure was notable for a single large diverticulum containing blood and blood clots with active bleeding in the second part of the duodenum. Two clips were placed, and 7 mL of epinephrine was injected into the site to achieve hemostasis. Patient was continued on a proton pump inhibitor on discharge and clopidogrel was resumed. Patient did not have reoccurrence of bleeding. Discussion: This case exhibits a rare cause of an upper GI bleed which can be easily treated via endoscopy. Typical differentials of upper GI bleeds are most commonly peptic ulcer disease, arteriovenous malformations, dieulafoy lesions, and gastritis however this case was unique as the patient had a diverticulum within the second portion of the duodenum. It is estimated that 0.14% of upper GI bleeding is caused by duodenal diverticula[2] .Hemostasis can be achieved by traditional methods like clipping and injecting of epinephrine. It is important to thoroughly visualize gastric and duodenal lumen during bleeding cases to find the source of bleeding. In conclusion despite common causes of upper GI bleeds a duodenal diverticulum should always be considered as a differential when the cause of an upper GI bleed is unknown.
Figure: Figure 1: Visible blood clot covering duodenal diverticulum with active bleeding
Figure: Figure 2: Duodenal diverticula clipped and injected with epinephrine.
Disclosures: Shivani Desai indicated no relevant financial relationships. Berhanu Geme indicated no relevant financial relationships.
Shivani K. Desai, MD1, Berhanu Geme, MD2. P0976 - When the Duodenum Surprises: Massive Hemorrhage from a Silent Diverticulum, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.