Urmimala Chaudhuri, DO1, Chase Thornton, MD2, Hassan Zreik, MD2, Drew Triplett, DO2 1Wright State University, Centerville, OH; 2Wright State University Boonshoft School of Medicine, Dayton, OH Introduction: Renal cell carcinoma (RCC) is the most common urogenital malignancy and carries the highest mortality with a rate of 30-40%. Around 400,000 cases of RCC are diagnosed per year and an estimated 20-33% present with metastases at diagnosis. Treatment for non-metastatic or localized disease is surgical resection; however, approximately 20- 50% will develop metastases despite resection. Metastasis typically involves the lungs, lymph nodes, bones, and liver. Colonic metastases is exceedingly rare. In this case report, we present a case of colonic metastasis from RCC.
Case Description/
Methods: An 80-year-old male with a history of left-sided RCC with known pulmonary and osseous metastasis presented with rectal bleeding, 40 lb unintentional weight loss over several months, and constipation. Hemoglobin on admission was 6.0 g/dL. CT imaging revealed a known solid mass of the left kidney and new wall thickening at the splenic flexure, raising concern for colonic malignancy. Gastroenterology (GI) was consulted, and colonoscopy revealed a tortuous, dilated colon and 2-3 cm ulcerated colonic nodule near the splenic flexure. Biopsies showed ulceration but no malignancy. The patient was discharged but returned one week later with recurrent rectal bleeding and hemoglobin of 5.5 g/dL. Flexible sigmoidoscopy revealed a friable, ulcerated colonic nodule with active bleeding. Hemostasis was achieved using epinephrine injection and two hemoclips. The lesion was resected via hot snare polypectomy. Pathology confirmed metastatic RCC. The patient declined surgical intervention after goals-of-care discussions and transitioned to hospice, passing away shortly thereafter. Discussion: Our case of colonic metastasis presents similarly to the majority of cases in the literature: a patient with known RCC presents with new onset rectal bleeding. While routine surveillance focuses on lungs, liver, and bone, colonic involvement should be considered in symptomatic patients. This case highlights the need for a high index of suspicion for GI metastasis in any RCC patient presenting with rectal bleeding.
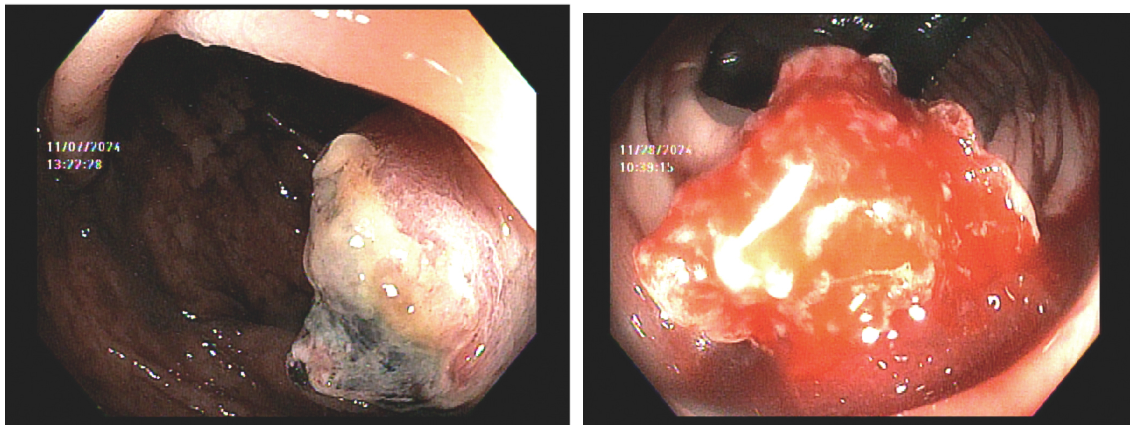
Figure: Endoscopic images of a metastatic renal cell carcinoma lesion at the splenic flexure. (Left) Ulcerated and nodular mass with necrotic areas. (Right) Friable, actively bleeding tumor visualized during repeat endoscopy
Disclosures: Urmimala Chaudhuri indicated no relevant financial relationships. Chase Thornton indicated no relevant financial relationships. Hassan Zreik indicated no relevant financial relationships. Drew Triplett indicated no relevant financial relationships.
Urmimala Chaudhuri, DO1, Chase Thornton, MD2, Hassan Zreik, MD2, Drew Triplett, DO2. P0974 - Colonic Metastasis of Renal Cell Carcinoma: A Rare Cause of Lower GI Bleed, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.