Saadia Jabbar, MD1, Nabiha Haider, DO2, Melchor Demetria, MD2 1Franciscan Health Olympia Fields, Homewood, IL; 2Franciscan Health Olympia Fields, Olympia Fields, IL Introduction: Aortoduodenal syndrome (ADS) is a rare condition described in fewer than 50 cases. It results from an abdominal aortic aneurysm (AAA) causing external compression of the duodenum, often the third portion. Management of ADS requires treatment of the AAA, typically via endovascular aneurysm repair (EVAR). With the rise in EVAR, complications like endoleaks are more frequently encountered. Among these, Type IIIc endoleaks, occurring at the interface between a bridging stent and a fenestrated graft, remain uncommon. To our knowledge, no case has previously linked a type IIIc endoleak to ADS presenting with upper gastrointestinal bleeding (UGIB).
Case Description/
Methods: An 80-year-old woman with a juxtarenal AAA previously treated with fenestrated EVAR and atrial fibrillation on Eliquis presented with abdominal pain and coffee-ground emesis. She was hemodynamically stable. Exam showed mild epigastric tenderness. Labs: hemoglobin 10.9 (baseline ~8.5), creatinine 1.6, INR 1.8. CT imaging revealed a 7.0 cm aneurysmal sac (sans rupture) compressing the duodenum, with associated gastric and esophageal distension. Aortography revealed a type IIIc endoleak at the renal artery stent. She underwent re-stenting, with full resolution of symptoms. Follow-up imaging showed aneurysm reduction to 6.3 cm. She was discharged tolerating a full diet. Discussion: This is the first reported case of ADS presenting as UGIB due to a type IIIc endoleak. While ADS usually presents with obstructive symptoms, this patient’s coffee-ground emesis suggested possible mucosal ischemia or reflux of pooled blood from duodenal compression. A comprehensive literature review reveals that very few ADS cases are associated with endoleaks, and fewer still to type IIIc or bleeding. This case highlights the importance of imaging and multidisciplinary care in identifying non-mucosal sources of GI symptoms. For gastroenterologists, it highlights the need to consider vascular postoperative complications, especially endoleaks, when evaluating unexplained UGIB in patients with prior EVAR.
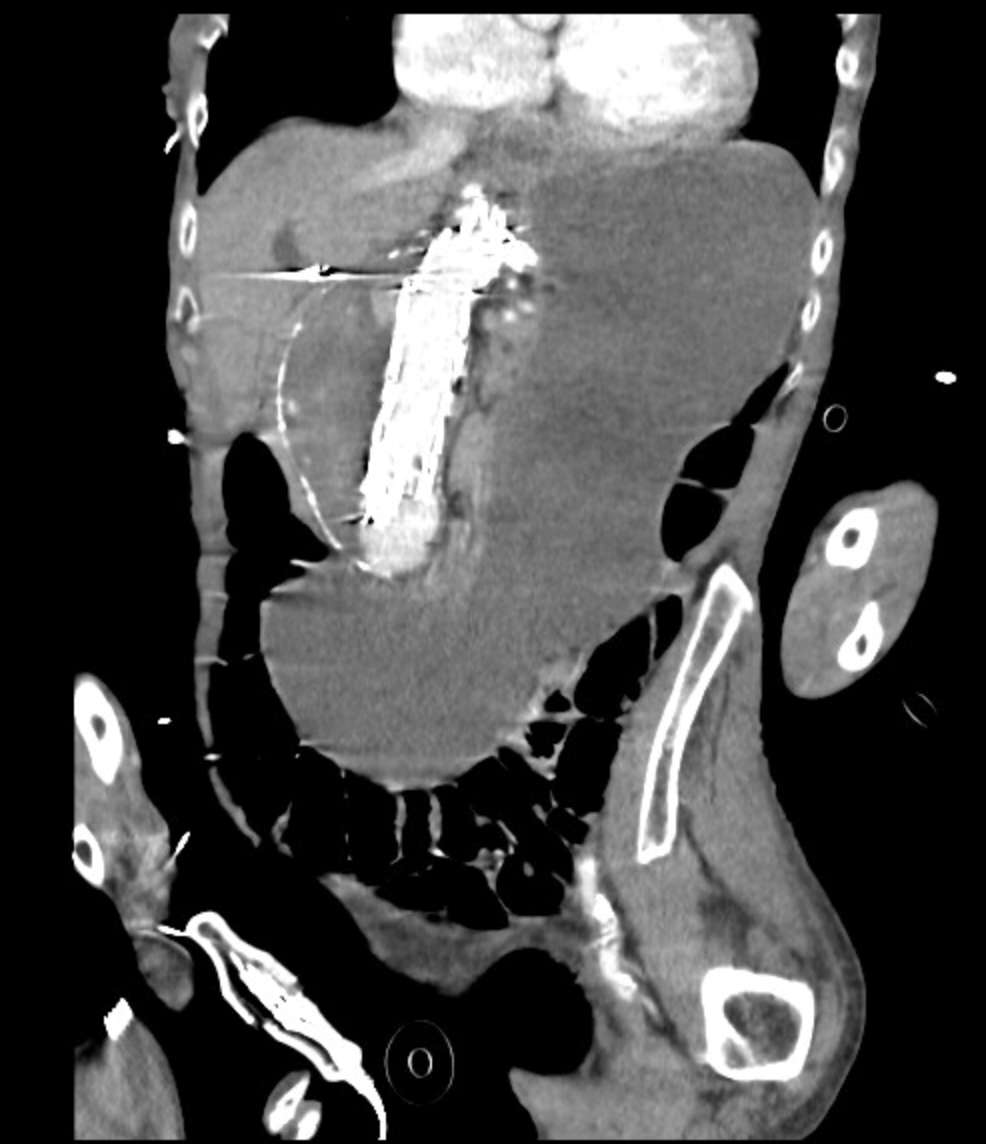
Figure: Coronal (Figure 1): CT images demonstrate a markedly enlarged juxtarenal abdominal aortic aneurysm (7.0 cm) causing extrinsic compression of the third portion of the duodenum, consistent with aortoduodenal syndrome. The presence of an endovascular stent graft with metallic artifact is noted, and the associated duodenal compression correlates with gastric and esophageal distension.
Figure: Axial (Figure 2): as mentioned above
Disclosures: Saadia Jabbar indicated no relevant financial relationships. Nabiha Haider indicated no relevant financial relationships. Melchor Demetria indicated no relevant financial relationships.
Saadia Jabbar, MD1, Nabiha Haider, DO2, Melchor Demetria, MD2. P0973 - Beyond Obstruction: A Unique Case of Aortoduodenal Syndrome Presenting With GI Bleeding, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.