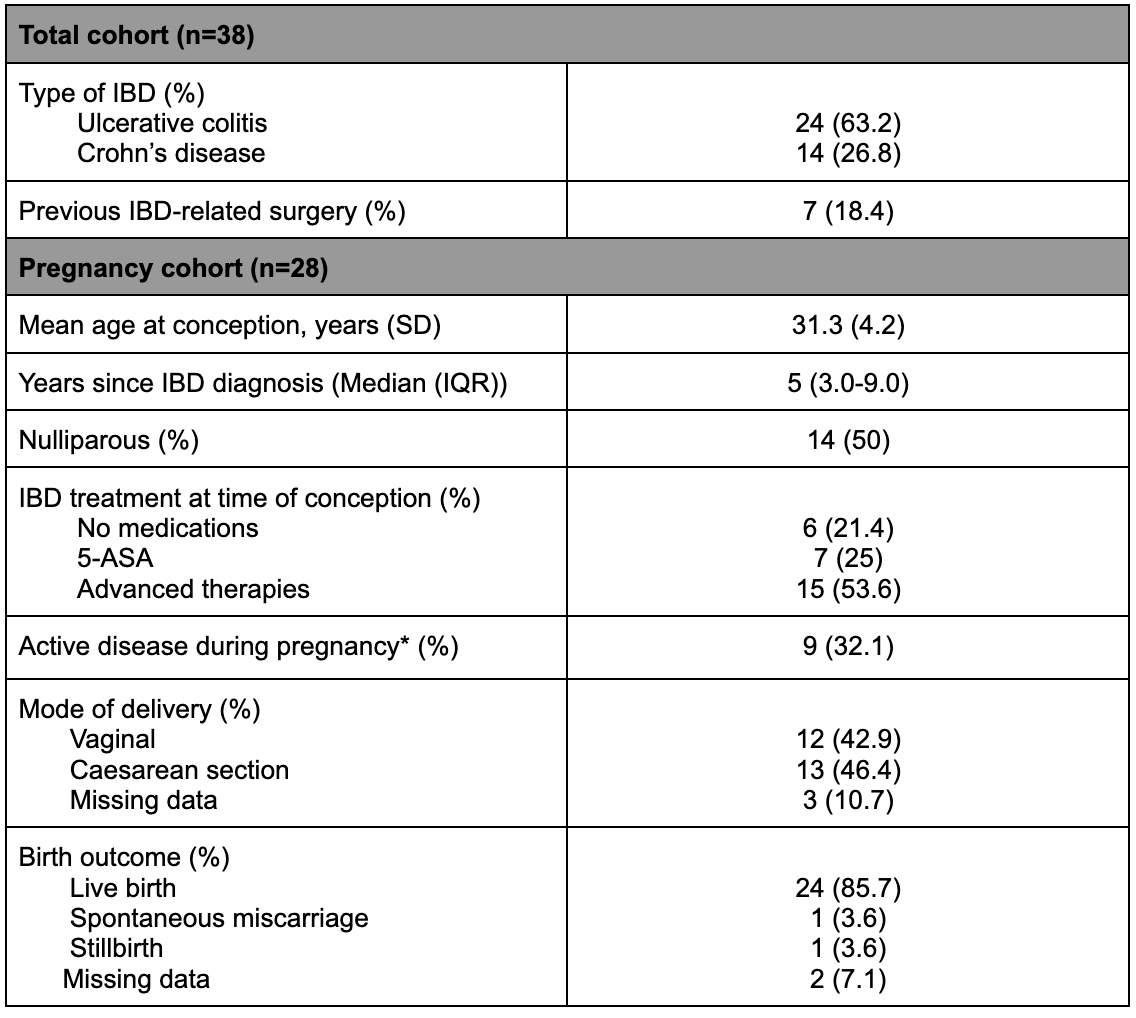
Jacquelin Blomker, MD1, Morgan Freeman, MD1, Ying Gibbens, MD, PhD2, Christopher Staley, PhD1, Eugenia Shmidt, MD1 1University of Minnesota, Minneapolis, MN; 2University of Minnesota Medical Center, Minneapolis, MN Introduction: Inflammatory bowel disease (IBD) and pregnancy are both conditions that are known to alter the microbiome. Currently, little investigation has been completed to understand the microbial profile in patients with IBD during pregnancy. Thus, we aim to evaluate the intestinal microbiome composition during pregnancy in those with IBD. Methods: Single-center prospective study of patients with IBD from our specialized IBD preconception clinic. Stool samples were collected before, during and after pregnancy, following informed consent. Microbiome analysis was performed using Shannon or Chao1 indices for alpha diversity and the Bray-Curtis dissimilarity index. Clinical information, pregnancy course and pregnancy outcomes were analyzed, with active disease during pregnancy defined by physician global assessment (PGA) score >1, need for steroids or change in IBD therapy. Results: Of the 38 participants in this study, 10 had preconception samples only and 28 were followed during pregnancy. Table 1 outlines patient characteristics and pregnancy outcomes. Of the 28, 9 (32.1%) had active disease during pregnancy. Time lapsed from IBD diagnosis to pregnancy was more brief in those who had an active disease as compared to those who did not have active disease (3 years vs. 6 years, P=0.047). Of patients on biologic therapy, 11% had active disease during pregnancy (11% vs 68%, P=0.013). Active disease during pregnancy was higher in those with ulcerative colitis (UC) as compared to those with Crohn’s disease (CD) (100% vs 0%, P</em>=0.029).
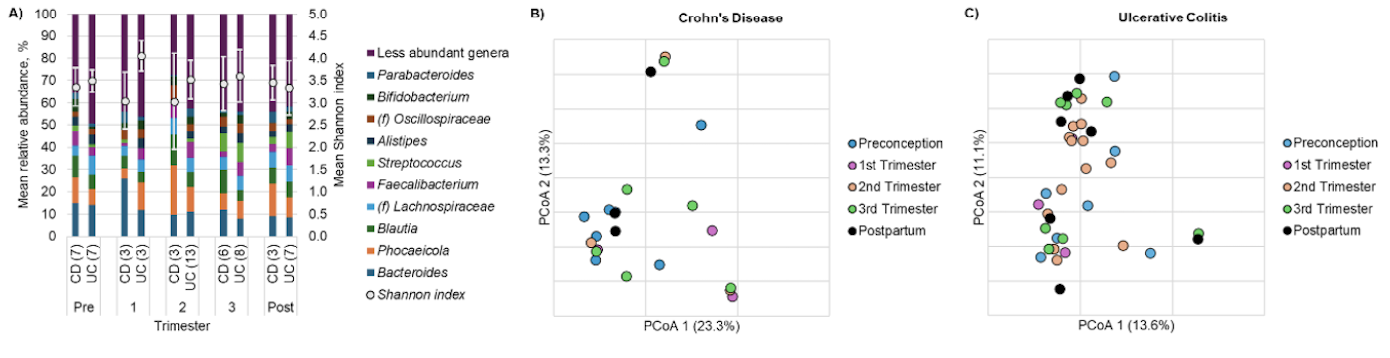
Predominant fecal microbial communities are shown in Figure 1A. Alpha diversity did not significantly change during pregnancy (Kruskal-Wallis P=0.687 and 0.081). Differences in community composition did not change significantly throughout pregnancy (analysis of similarity R=-0.009, P=0.58). Differences between UC and CD patients were noted in the 1st trimester. Those with UC showed greater alpha diversity and greater relative abundances of Alistipes and Faecalibacterium but lower abundances of Bacteroides (P < 0.05). There were no differences between IBD types in the 2nd or 3rd trimesters. Discussion: Our study supports previous findings of differences in microbiome composition between UC and CD patients early in pregnancy. Additionally, the use of biologic therapy is a protective factor against active disease during pregnancy. Future work should include larger cohorts to further analyze the microbiome and its correlation with IBD factors associated with pregnancy outcomes.
Figure: Table 1. Baseline characteristics of patients with IBD during pregnancy *Active disease defined by physician global assessment (PGA) score >1, need for steroids or change in IBD therapy during pregnancy
Figure: Figure 1. Microbial diversity and composition in pregnancy-associated fecal samples. A) Distribution of predominant genera and Shannon indices. B) Principal coordinate analysis of Bray-Curtis dissimilarities among samples from patients with CD. C) Principal coordinate analysis of Bray-Curtis dissimilarities among samples from patients with UC
Disclosures: Jacquelin Blomker indicated no relevant financial relationships. Morgan Freeman indicated no relevant financial relationships. Ying Gibbens indicated no relevant financial relationships. Christopher Staley indicated no relevant financial relationships. Eugenia Shmidt: Bristol Myers Squibb – Grant/Research Support.
Jacquelin Blomker, MD1, Morgan Freeman, MD1, Ying Gibbens, MD, PhD2, Christopher Staley, PhD1, Eugenia Shmidt, MD1. P1169 - Profile of the Intestinal Microbiome of Inflammatory Bowel Disease During Pregnancy, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.