Sanjana Verma, MD The Johns Hopkins Hospital, Baltimore, MD Introduction: Sweet syndrome (SS), or acute febrile neutrophilic dermatosis, is a rare inflammatory condition characterized by sudden onset of fever, painful erythematous or purpuric cutaneous lesions, and neutrophilic infiltration in the affected tissues. It is often associated with systemic diseases, such as autoimmune conditions, infections, or malignancies.
Case Description/
Methods: A 70-year-old female with a history of ulcerative colitis (UC) on mesalamine presented with a two-week history of progressive eyelid swelling, oral ulcerations, and skin lesions. Her symptoms began with bilateral periorbital swelling with yellow drainage, followed by painful, honey-crusted plaques on the lower lip, inner left cheek, upper palate, and scalp. She later developed a dark, non-tender lesion on the left calf and an erythematous ulceration on the right calf. On presentation, she was febrile, and workup revealed a leukocytosis with neutrophilic predominance and elevated inflammatory markers. Imaging of the lower extremities and chest/abdomen/pelvis showed soft tissue changes concerning for cellulitis and suggested possible infectious or inflammatory colitis. Ophthalmology, infectious disease, and dermatology services were consulted. Punch biopsies of the calf and scalp lesions revealed a dense neutrophil-rich infiltrate without vasculitis, consistent with SS. Gastroenterology was consulted for endoscopic evaluation given overall concern that her underlying UC or occult malignancy was the primary driver of her presentation. Colonoscopy showed patchy areas of severe erythema and ulceration in the cecum, ascending, transverse, and descending colon with pathology consistent with active UC. She was initiated on intravenous steroids for SS after infectious work up showed no growth at 48 hours. Shortly after initiation, she had a reduction in her lesions, ophthalmic symptoms, and inflammatory markers. She was ultimately discharged on an oral prednisone taper with a plan to switch mesalamine to infliximab outpatient. Discussion: This case of SS is notable for its association with UC, which is less commonly implicated than Crohn’s disease, and for its rare oral and ocular involvement. It emphasizes the need for clinicians to consider SS in patients with inflammatory bowel disease who present with atypical skin lesions, fever, and elevated inflammatory markers, highlighting the importance of a multidisciplinary approach to ensure proper diagnosis and treatment.
Figure: Lower lip ulcerations with hemorrhagic and yellow crust
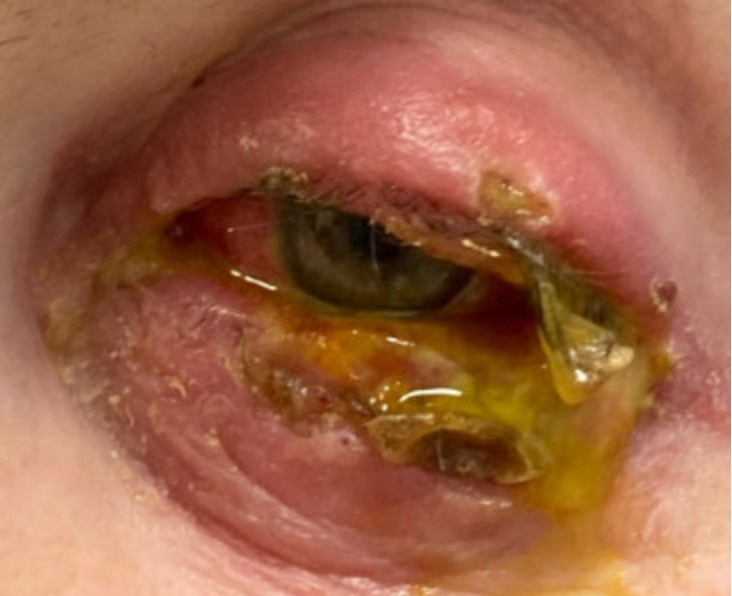
Figure: Left eye ulceration with copious yellow drainage and conjunctival injection
Disclosures: Sanjana Verma indicated no relevant financial relationships.
Sanjana Verma, MD. P1249 - Beyond the Colon: Sweet’s Syndrome as a Complication of Ulcerative Colitis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.