Colton J. Hartig, MD, Muna Shakhashiro, MD, Thein Myint, MBBS, Nathan Shelman, MD University of Kentucky, Lexington, KY Introduction: Cytomegalovirus (CMV) infection is generally asymptomatic in immunocompetent patients. If symptomatic, CMV can cause a mononucleosis-like syndrome characterized by fever, fatigue, and lymphadenopathy. Rarely, CMV can cause colitis in healthy patients. Diagnosis of CMV colitis requires detection of CMV inclusions or positive CMV-specific immunohistochemistry staining on tissue biopsy.
Case Description/
Methods: A 53-year-old female who works in a primary care clinic with a history of IBS-D, psoriatic arthritis, and Hashimoto’s thyroiditis presented with three weeks of headache and fever. Upon admission, lab testing showed AST 74 U/L, ALT 90 U/L, total bilirubin 0.5 mg/dL, and platelets 148,000/µL. Blood cultures, viral hepatitis panel, and cerebrospinal fluid analysis were negative. CT showed mild hepatic steatosis. On hospital day 3, the patient developed profuse watery diarrhea. GI PCR and stool testing for ova and parasites were negative. At this point, the differential diagnosis included viral infections such as HIV, CMV, EBV, HSV, and VZV. CMV viremia was detected at 97,000 copies/ml. A colonoscopy was performed, notable for multiple ulcerations in the cecum and ascending colon (figure 1). Biopsies from the affected areas were positive for CMV cytopathic effect and CMV-specific immunohistochemistry staining (figure 2). Testing for immunocompromising conditions such as HIV was negative. The patient was treated with IV ganciclovir, followed by oral valganciclovir for a total of 21 days with resolution of CMV viremia. At two-month follow up, the patient’s diarrhea resolved to her baseline of three episodes of watery diarrhea daily. Fecal calprotectin, TSH, fecal ova and parasite panel, CRP, and celiac disease testing were within normal limits. Discussion: CMV colitis in immunocompetent patients is uncommon. Although she had a history of psoriatic arthritis, she had not taken immunosuppressive medications for over 15 months. CMV reactivation in healthy patients can occur during episodes of acute illness, however this patient was not initially acutely ill from another source. Since this patient works in a primary care clinic, she may have had an occupational exposure to CMV. Ultimately, it is unclear why this patient developed such a severe manifestation of CMV disease and her course represents a unique case of CMV in an immunocompetent patient. CMV colitis should be considered in immunocompetent patients with diarrhea and transaminitis after exclusion of common etiologies of infectious diarrhea.
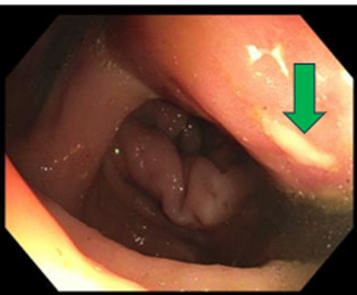
Figure: Figure 1. Endoscopic findings. Superficial aphthous ulcer in the cecum (green arrow).
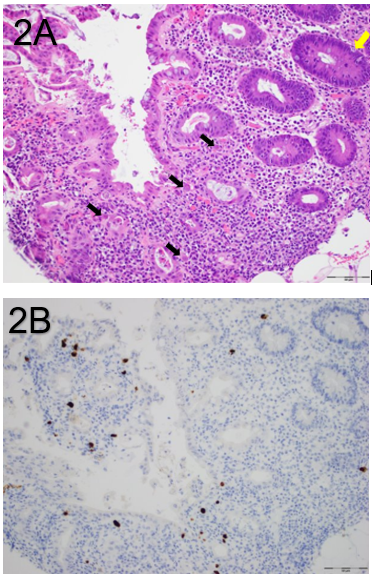
Figure: Figure 2. Histopathological findings of the cecum. (2A) Mixed inflammation with scattered crypt apoptosis (yellow arrow) and numerous stromal and endothelial cells with viral cytopathic effect (black arrows). (2B) Numerous stromal and endothelial cells immunoreactive for CMV immunohistochemistry staining.
Disclosures: Colton Hartig indicated no relevant financial relationships. Muna Shakhashiro indicated no relevant financial relationships. Thein Myint indicated no relevant financial relationships. Nathan Shelman indicated no relevant financial relationships.
Colton J. Hartig, MD, Muna Shakhashiro, MD, Thein Myint, MBBS, Nathan Shelman, MD. P1317 - CMV Mononucleosis Complicated by Viremia and Colitis in an Immunocompetent Patient, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.