University Hospital Düsseldorf Düsseldorf, Nordrhein-Westfalen, Germany
Award: ACG Presidential Poster Award
Esma Zeynep Kizilaslan, MD, Sven Heiko Loosen, MD, Sinan Kalmuk, MD, Wolfram Knoefel, MD, Tom Luedde, PhD, Jennis Kandler, MD University Hospital Düsseldorf, Düsseldorf, Nordrhein-Westfalen, Germany Introduction: In patients with Roux-en-Y gastric bypass (RYGB), conventional ERCP is not possible due to altered anatomy. Alternatives include EUS-directed transgastric ERCP (EDGE), laparoscopic-assisted ERCP (LA-ERCP), and enteroscopic ERCP (E-ERCP). EDGE is a technique that creates a temporary fistula between the gastric pouch and the excluded stomach using a lumen-apposing metal stent (LAMS), allowing conventional ERCP. While EDGE is effective in RYGB cases, its use in patients with a prior sleeve gastrectomy (SG) converted to RYGB (SG-RYGB) is rare due to limited working space in the reduced stomach sections. We present a case of successful EDGE following failed alternative approaches.
Case Description/
Methods: A 64-year-old woman with a history of SG-RYGB for morbid obesity underwent a cholecystectomy for symptomatic cholelithiasis at an external hospital. Due to postoperative cystic duct stump leakage and untreated bile duct stones, LA-ERCP was performed, resulting in the placement of a pancreatic stent (PS) but failed biliary cannulation, prompting her transfer to our surgical center. Exploratory laparotomy with common bile duct (CBD) exploration and partial stone removal was conducted, but bile leakage persisted. Conservative measures, including CT-guided drainage of a bilioma in the former gallbladder bed and antibiotics, were unsuccessful. Therefore, the patient was referred to our Interventional Endoscopy Unit (Department of Gastroenterology), and EDGE was performed. Using a therapeutic linear echoendoscope, the excluded stomach was punctured with a 19-gauge EUS needle, followed by the injection of contrast media to confirm positioning. Subsequently, sterile water was injected to distend the excluded stomach. A 0.035” guidewire was advanced, followed by the placement of a 20×10 mm electrocautery-enhanced LAMS, creating a gastro-gastric fistula. Transgastric ERCP showed large CBD stones, a cystic duct stump leak, and the PS. After biliary sphincterotomy, all stones were extracted, a 10 French biliary plastic stent was placed, and the PS was extracted. No complications occurred. After healing of the bile leak, the biliary stent and LAMS were removed. Discussion: This case illustrates the value of EDGE for biliopancreatic interventions in RYGB patients, even after conversion from SG, which increases procedural complexity. In tertiary centers, it should be considered early in post-bariatric patients.
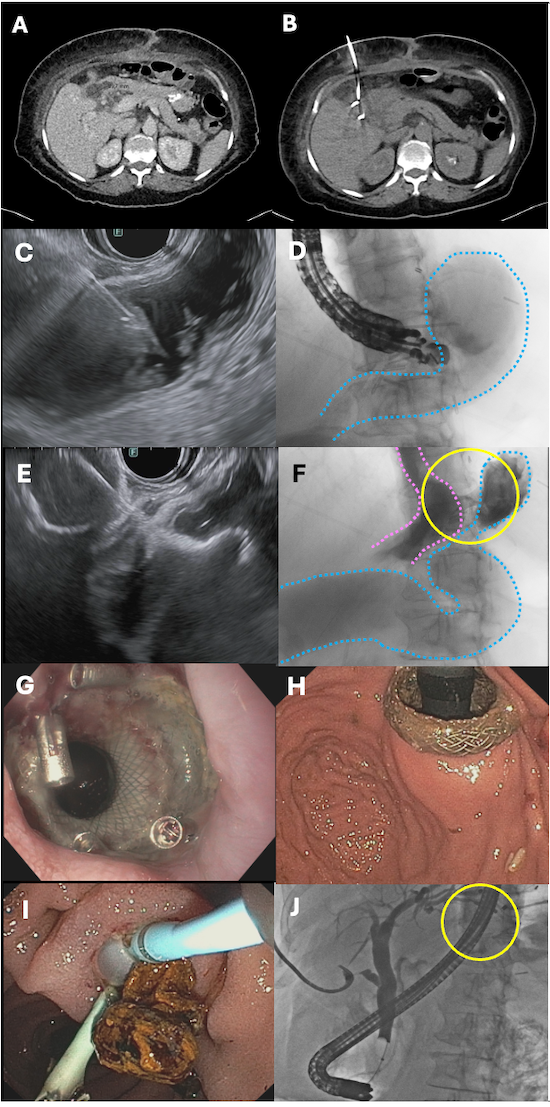
Figure: Fig. 1 EDGE in a patient after conversion from sleeve gastrectomy to RYGB. ERCP was indicated due to biliary stones, bile leakage after laparoscopic cholecystectomy, failed biliary cannulation during LA-ERCP at an external hospital, and unsuccessful surgical CBD revision. (A) CT scan showing a 3.9 × 2.0 × 2.1 cm bilioma in the former gallbladder bed. (B) CT-guided percutaneous drainage of the bilioma. (C) EUS-guided puncture of the excluded stomach using a 19G FNA needle (EUS image). (D) Fluoroscopic image of the puncture. The blue line marks the excluded stomach filled with diluted contrast media. (E) EUS showing correct placement of the LAMS. (F) Fluoroscopy showing the gastro-gastric fistula without contrast leakage. Blue line: excluded stomach; pink line: gastric pouch; yellow circle: LAMS position. (G) Endoscopic view of the LAMS fixed with clips (antegrade view). (H) Retroflex endoscopic view of the LAMS during transgastric ERCP. (I) ERCP with stone extraction after sphincterotomy. (J) Final cholangiogram showing a dilated CBD without residual stones and leakage from the cystic duct stump; percutaneous drain in place. Yellow circle: LAMS.
Disclosures: Esma Zeynep Kizilaslan indicated no relevant financial relationships. Sven Heiko Loosen indicated no relevant financial relationships. Sinan Kalmuk indicated no relevant financial relationships. Wolfram Knoefel indicated no relevant financial relationships. Tom Luedde indicated no relevant financial relationships. Jennis Kandler indicated no relevant financial relationships.
Esma Zeynep Kizilaslan, MD, Sven Heiko Loosen, MD, Sinan Kalmuk, MD, Wolfram Knoefel, MD, Tom Luedde, PhD, Jennis Kandler, MD. P1469 - EUS-Directed Transgastric ERCP (EDGE) After Conversion of Sleeve Gastrectomy to Roux-en-Y Gastric Bypass (SG-RYGB): Managing Biliary Leak and Stones in Complex Surgically Altered Anatomy, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.


 photo")