University of Alabama at Birmingham Birmingham, AL
Carter Edmunds, MD1, Lindsay Duy, MD2, Kelly Hammoudi, PA-C2, Swati Pawa, MD3 1University of Alabama at Birmingham, Birmingham, AL; 2Atrium Health Wake Forest Baptist, Winston-Salem, NC; 3Atrium Health Wake Forest Baptist,, Winston-Salem, NC Introduction: Afferent loop syndrome (ALS) is a rare complication following upper gastrointestinal tract reconstruction surgery, such as gastrojejunostomy or pancreaticoduodenectomy. It occurs from obstruction of the afferent limb, with potential causes including adhesions, malignancy, anastomotic strictures, or hernias. We present a unique case of ALS with bowel obstruction, obstructive jaundice, and pancreatitis, managed by EUS-guided gastroenterostomy (EUS-GE) with lumen-apposing metal stent (LAMS).
Case Description/
Methods: A 69-year-old female with a Whipple resection for cholangiocarcinoma 3 years prior presented with abdominal pain, nausea, and vomiting. The patient had right upper quadrant tenderness on exam and elevated liver enzymes and lipase.
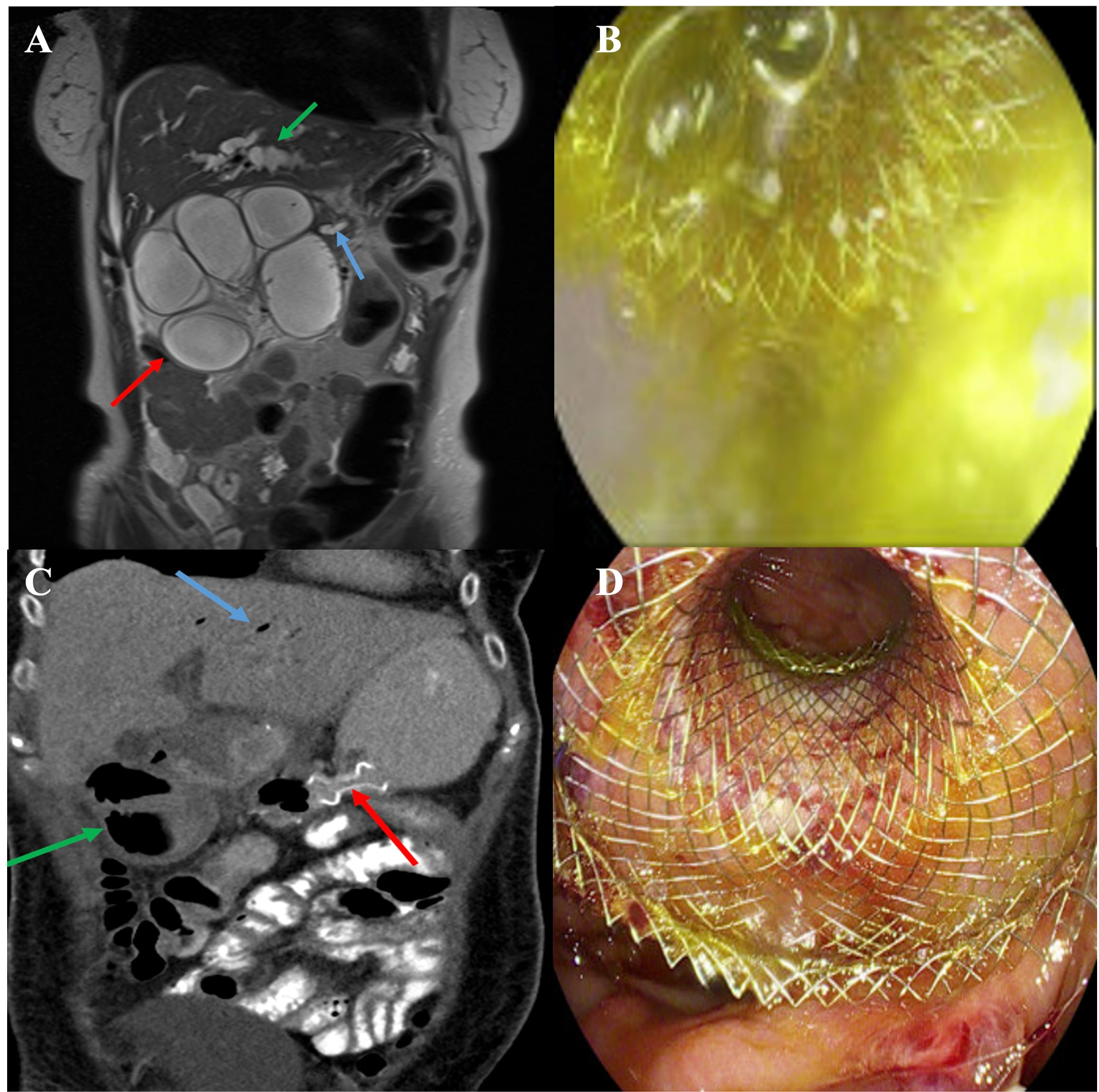
An MRI showed evidence of pancreatitis and an obstruction to the proximal blind-ending afferent limb distal to both the pancreatic jejunostomy and hepaticojejunostomy anastomoses. The intrahepatic and pancreatic ducts were dilated, but the hepaticojejunostomy anastomosis was patent, concerning for obstructed hepatobiliary limb (Fig. 1A). Push enteroscopy was pursued, but the endoscope could not be advanced beyond the strictured afferent limb. An EUS- GE was performed and LAMS was placed under endoscopic and fluoroscopic guidance with drainage of large amount of bile (Fig. 1B). Follow-up CT showed LAMS in proper placement between the stomach and afferent limb and decreased dilation of the afferent limb (Fig. 1C). Patient’s bowel obstruction symptoms subsequently resolved, and her liver enzymes normalized. One month later, the patient’s symptoms returned, and a repeat EGD showed a dislodged LAMS in the stomach with similar CT scan findings of ALS. Subsequent EUS-GE was performed to place a LAMS (via transgastric approach) in the afferent limb, and the placement was confirmed via fluoroscopy. The LAMS was placed in the afferent limb, affixed to the stomach with endo sutures. (Fig. 1D). Discussion: This case highlights a rare but significant presentation of afferent loop syndrome causing simultaneous small bowel obstruction, obstructive jaundice, and pancreatitis. Although each complication can occur independently, they rarely occur in combination. EUS-GE is a minimally invasive alternative to surgical bypass. However, stent migration can occur, as in our case, requiring repeat LAMS placement and suture affixation. More studies are needed to determine optimal intervention in such cases.
Figure: Figure 1. A) MRI shows an abnormally dilated afferent loop (red arrow). The pancreatic duct (blue arrow) and intrahepatic biliary ducts are dilated (green arrow). B) Endoscopic view of bile drainage of LAMS deployment in the afferent limb. C) CT image after successful axios stent placement from the stomach to afferent loop (red arrow). There is decompression of bowel loops with air (green arrow). There is also expected pneumobilia (blue arrow). D) Endoscopic view of the proximal phalange of the lumen-apposing metal stent.
Disclosures: Carter Edmunds indicated no relevant financial relationships. Lindsay Duy indicated no relevant financial relationships. Kelly Hammoudi indicated no relevant financial relationships. Swati Pawa: Boston Scientific – Consultant.
Carter Edmunds, MD1, Lindsay Duy, MD2, Kelly Hammoudi, PA-C2, Swati Pawa, MD3. P1462 - Afferent Loop Syndrome Presenting With Bowel Obstruction, Obstructive Jaundice, and Pancreatitis Managed by EUS-Guided Gastroenterostomy, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.