Scot M. Lewey, DO, FACG1, Neil Sharma, MD, FACG2, Jason Tcheng, MD3, Meghan Riley, MD4 1Banner Health, Fort Collins, CO; 2Banner Health, Phoenix, AZ; 3Banner MD Anderson, Greeley, CO; 4Summit Pathology, Fort Collins, CO Introduction: Differential diagnosis of PET positive paresphageal lesions includes a variety of malignant etiologies. Both gastrointestinal stromal tumors (GIST, that have malignant potential, and Schwannomas that very rarely do can be PET positive. Fine needle aspiration (FNA) biopsies historically have had variable success in obtaining accurate pathologic diagnosis in GIST and Schwannomas.
Case Description/
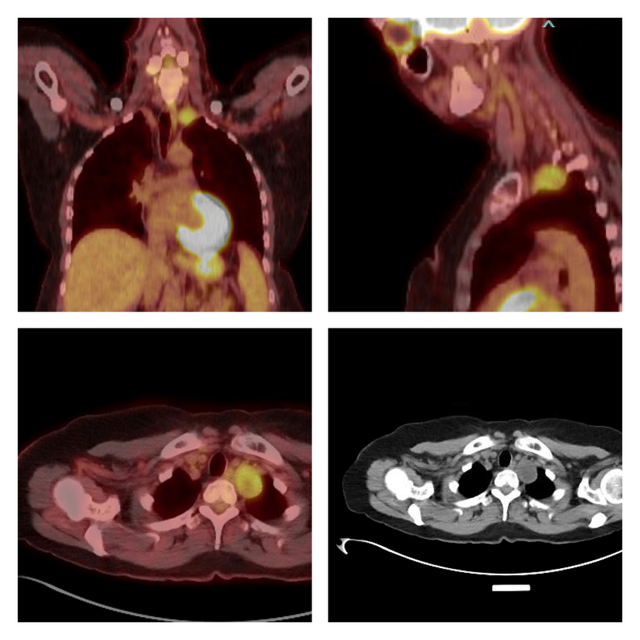
Methods: 55-year-old Caucasian woman with a past history of migraines, depression and schizophrenia underwent diagnostic imaging after a 3-month history of left ear fullness, intermittent dizziness and a change in her usual migraine headache pattern. Contrast enhanced computed tomography (CT) of head and neck revealed a 3 cm solid soft tissue mass along the left posterior thoracic inlet near but not involving the esophagus. Family history was remarkable for lung cancer, ovarian cancer, and non-Hodgkin’s lymphoma. Genetic testing had previously revealed heterozygosity for MSHE del exons 4-8. Social history was negative for tobacco, alcohol, or elicit drug use but positive for marijuana use 1-2 times per month. A normal physical exam with a body mass index 29.4 was noted followed by a Fluorine-18 fluorodeoxyglucose positron emission tomography scan (PET) revealed an well circumscribed ovoid mass in the left thoracic inlet with central low attenuation but high attenuation around the periphery (see image 1) measuring 3.2 cm and moderately intense FDG uptake at a max SUV of 4.5. Relatively diminished uptake was seen centrally suggesting cystic change or necrosis. Curvilinear EUS exam revealed a well circumscribed ovoid heterogeneously hypoechoic lesion with some focal anechoic cystic appearance centrally and a marginal halo in the left paraesophageal region (image 2). EUS directed core biopsy was performed with a 22-gauge Franseen needle. A benign spindle cell Schwannoma was confirmed with special stains positive for S100, SOX-10 and CD56 but negative for Pankeratin, Calretinin, CD34, Desmin, DOG1 and CD117.
Discussion: The differential diagnosis of PET positive paraesopnageal lesions includes metastatic malignancies, lymphoma, GIST and Schwannomas. Imaging features are not reliable for confirming the etiology of such lesions. On EUS both GIST and Schwannomas are typically heterogeneously hypoechoic often with focal cystic changes but a marginal halo is more typical of a Schwannoma. EUS FNB core biopsies of extraesophageal PET positive lesion can be confirmatory of etiology.
Figure: PET CT Images of Paraesophageal Schwannoma
Figure: EUS Image of Paraesoophageal Schannoma
Disclosures: Scot Lewey indicated no relevant financial relationships. Neil Sharma: Boston Scientific – Consultant. Medtronic – Consultant. Nanology – Consultant. Olympus – Consultant. Steris – Consultant. Jason Tcheng indicated no relevant financial relationships. Meghan Riley indicated no relevant financial relationships.
Scot M. Lewey, DO, FACG1, Neil Sharma, MD, FACG2, Jason Tcheng, MD3, Meghan Riley, MD4. P1458 - Endosonographic (EUS) Fine Needle Biopsy of a Paraesophageal PET Positive Lesion, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.