William Dungan, MD1, Mason Adams, MD2 1University of South Alabama, Mobile, AL; 2USA Health, University of South Alabama, Mobile, AL Introduction: Endovascular coil embolization is an effective treatment for life-threatening gastrointestinal bleeding. Known complications include access site injury, bowel ischemia, infection, and rebleeding. Coil migration is exceedingly rare, particularly into the biliary tree, which may lead to strictures, stone formation, and cholangitis. We present a rare case of coil migration into the common bile duct (CBD) resulting in obstructive choledocholithiasis, managed endoscopically.
Case Description/
Methods: A 71-year-old female with coronary artery disease on clopidogrel and prior duodenal ulcer treated with gastroduodenal artery embolization presented with cholestatic liver injury on routine follow-up. Six months earlier, she underwent coil embolization for a bleeding duodenal ulcer. She denied abdominal pain, jaundice, fever, alcohol, or supplement use. Vitals were stable, exam unremarkable. Labs: total bilirubin 0.7 mg/dL, alk phos 1054 U/L, AST 102 U/L, ALT 188 U/L. Ultrasound revealed CBD dilation and gallbladder sludge. MRCP showed a 1.2 cm CBD with a filling defect. ERCP identified a large distal CBD stone and adjacent embolization coils. Sphincterotomy and balloon sphincteroplasty were performed with biliary stent placement due to stricture and difficulty accessing the duct. While liver tests improved initially, they worsened prior to discharge. Repeat ERCP revealed stent occlusion and persistent stone. Further balloon dilation enabled stone extraction, exposing metallic coils eroding into the CBD. Cholangioscopy with coil removal was deferred due to recent clopidogrel use. A multidisciplinary discussion with interventional radiology and surgery was held. One week later, ERCP with balloon sweeps and retrieval using rat-toothed and pediatric forceps enabled successful coil extraction without complication. The patient was discharged in stable condition. Discussion: Coil migration into the biliary tree is rare (< 1%), typically following hepatic artery embolization or hepatobiliary surgery. Resultant obstruction, cholangitis, or stone formation may occur months to years later. ERCP is the preferred diagnostic and therapeutic modality, though efficacy may be limited by ductal stricture or stone burden. Adjunctive tools include cholangioscopy, lithotripsy, or specialized forceps. Invasive approaches such as percutaneous cholangioscopy or surgical exploration may be necessary when endoscopy fails. Our case highlights endoscopic coil retrieval as a feasible and effective first-line treatment strategy.
Figure: Figure 1. Fluoroscopic Imaging of Coil Migration into the Biliary Tree Radiographic fluoroscopy during ERCP revealing migrated embolization coils within the CBD. (Left) Coils seen embedded along the CBD wall prior to intervention. (Right) Cholangiogram showing biliary tree dilation, CBD filling defect, and embedded coils, consistent with obstructive choledocholithiasis.
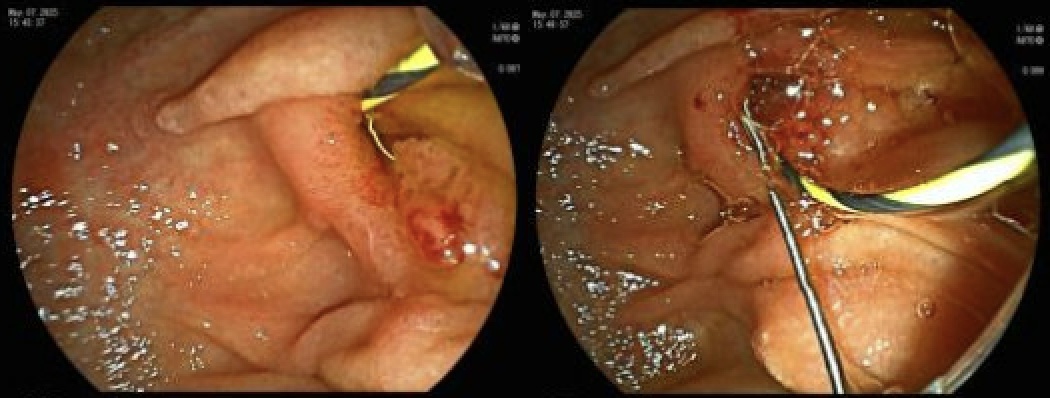
Figure: Figure 2. Endoscopic Coil Retrieval from the Common Bile Duct Endoscopic views demonstrating coil erosion into the distal CBD. (Left) Initial visualization of exposed metallic embolization coil within the CBD. (Right) Successful retrieval during ERCP.
Disclosures: William Dungan indicated no relevant financial relationships. Mason Adams indicated no relevant financial relationships.
William Dungan, MD1, Mason Adams, MD2. P1457 - Coilodocholithiasis: ERCP Management of Biliary Obstruction from Gastroduodenal Artery Coil Migration, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.