University of Arizona College of Medicine, Phoenix Phoenix, AZ
Vanessa Eller, MD1, Kevin Liu, MD2 1University of Arizona College of Medicine, Phoenix, Phoenix, AZ; 2Banner University Medical Center, Phoenix, AZ Introduction: Esophageal perforations are associated with significant morbidity and mortality, requiring complex multidisciplinary co-management with surgery, interventional gastroenterology and interventional radiology. Endoscopic therapies for treatment of perforations include clip placement, enteral stenting, endoscopic suturing and endovacuum therapy (EVT).
We report on a large ( >15 cm) perforation cavity in thesetting of proximal esophageal perforation secondary to trauma from a gunshot wound that was treated primarily with EVT and resulted in successful closure.
Case Description/
Methods: A 20-year-old patient presented as a trauma with four gunshot wounds in the neck and posterior trunk. He was emergently transported to the OR and underwent clamshell thoracotomy where he was found to have a blast injury through the trachea and proximal esophagus with a 3 cm full thickness defect. The esophageal injury was primarily repaired and buttressed with an intercostal muscle flap.
Three weeks after initial repair, there was dehiscence of his repair. On endoscopy, the 15 mm full thickness defect in the proximal esophagus was sutured with closure of the perforation. Subsequent dehiscence of the repair led to the decision to proceed with EVT. The perforation was intubated and a large contaminated mediastinal cavity ( >15 cm in size) was visualized. After the cavity was cleared of debris, EVT was initiated. In total, the patient underwent10 EVT exchanges over 3 months. Initially, EVT was placed intracavitary (within the perforation cavity). As the cavity granulated and decreased in size, EVT was placed intraluminally (with the sponge in the esophagus opposed to the perforation). The cavity had significantly reduced in size to 1-2 cm. A fully covered metal stent was placed across the residual defect and left for two months. After removal, the perforation had completely healed with no leak visualized on esophagram. Discussion: EVT is an effective endoscopic tool for management of esophageal perforations and leaks. By applying negative pressure to the defect, it promotes drainage and granulation of the defect. There is currently limited endoscopic equipment available for EVT and sponges must be manually created by suturing surgical wound vacuum sponges to nasogastric tubes. For perforations associated with a large, contaminated perforation cavity or leak as in this case, EVT may be more useful than other endoscopic techniques as it promotes healing of the cavity in addition to closure of the perforation.
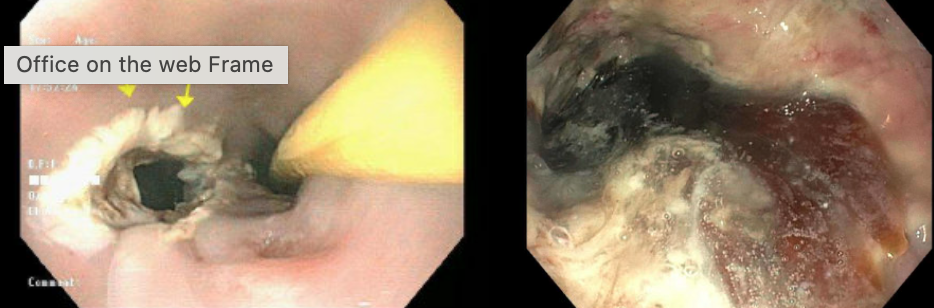
Figure: Left: Perforation on initial endoscopy Right: Perforation cavity in mediastinum with purulent fluid and retained surgical material
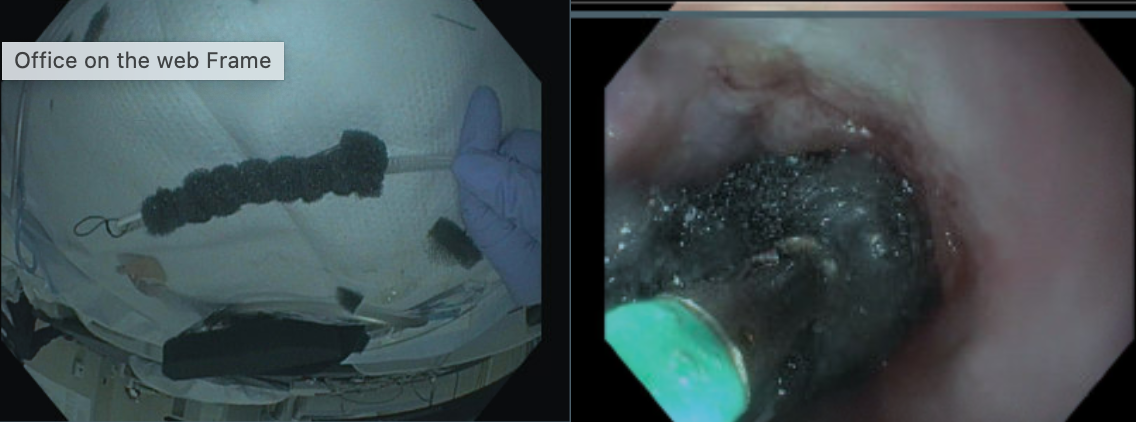
Figure: Left: Endovacuum sponge Right: Placement of endovacuum sponge into the perforation cavity
Disclosures: Vanessa Eller indicated no relevant financial relationships. Kevin Liu indicated no relevant financial relationships.
Vanessa Eller, MD1, Kevin Liu, MD2. P1454 - Endovacuum Therapy of Massive Esophageal Perforation Following Penetrating Thoracic Trauma: A Case Report, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.