Christopher G Ortiz-Morales, MD1, Sofia I. Frau Rivera, MD2 1Sistema de Salud Memonita - Cayey, Humacao, Puerto Rico; 2Sistema de Salud Menonita - Cayey, Coamo, Puerto Rico Introduction: Bouveret syndrome is a rare type of gallstone ileus, characterized by gastric outlet obstruction caused by a gallstone lodged in the distal stomach or proximal duodenum. It results from chronic gallbladder inflammation leading to a biliary-enteric fistula. Typically, it presents with nonspecific symptoms, most commonly epigastric pain, nausea with abdominal pain and distention. The standard treatment involves a surgical procedure, though it carries a higher mortality rate. Bouveret syndrome accounts for only 1–3% of gallstone ileus cases, with just over 300 cases reported as of 2022. We report the first case in Puerto Rico of this pathology in a nonagenarian patient with classic symptomatology, further complicated by pre-existing conditions.
Case Description/
Methods: A 91-year-old female with a history of Alzheimer’s disease, type 2 diabetes, hypertension, and cholecystitis presented to the emergency department with persistent diarrhea, nausea, and vomiting. Physical examination revealed severe malnutrition with right upper and lower quadrant pain. Laboratories showed leukocytosis (26.74 x 10^9/L) with normal liver function. Diagnosis of duodenal obstruction and gastroenteritis was established by imaging, revealing obstruction secondary to large gallstone formation, consistent with Bouveret syndrome. Given the patient's age and comorbidities, an endoscopic retrograde cholangiopancreatography (ERCP) was performed. During the exploratory part of the procedure, an impacted large gallstone (4.7cm) was identified at the third portion of the duodenum. Removal of the gallstone with the use of endoscopic tools was unsuccessful. Laser lithotripsy was subsequently employed, fragmenting the stone into multiple large pieces. A significant amount of the gallstone fragments could not be removed. An abdominopelvic CT was scheduled to revise their anatomical position. Imaging showed two significant gallstone fragments, located proximally and distally at the jejunum. Post-procedure course was uneventful. Discussion: Bouveret syndrome's rarity highlights the importance of its awareness and early recognition, as a delayed treatment could lead to increased morbidity and mortality. Treatment strategies should be individualized to the patient’s clinical condition and comorbidities. In elderly patients, where surgery may pose significant risks, non-surgical options such as laser lithotripsy, a minimally invasive technique that fragments the gallstone with minimal risks to adjacent tissues, should be considered.
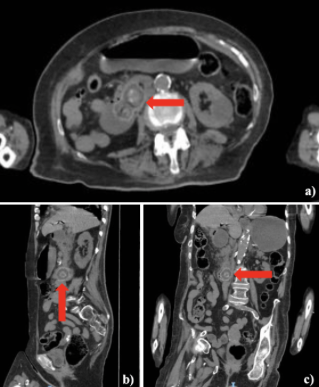
Figure: Figure 1. Abdominopelvic CT performed identified the gallstone located at the third part of the duodenum. a) Axial view. b) Sagittal view. c) Coronal view. Rounded heterogeneous densities in the third portion of the duodenum.
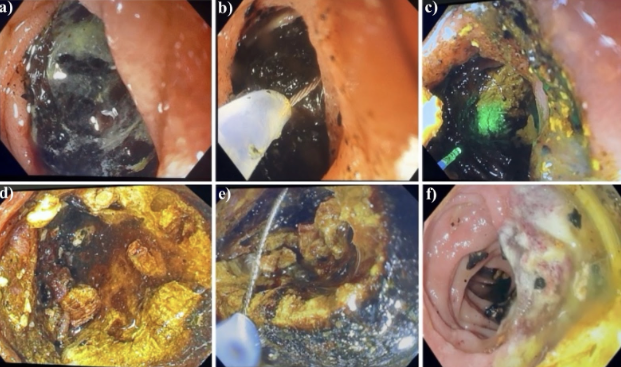
Figure: Figure 2. Endoscopic images of the procedure a) Fixed gallstone. b) Attempt of gallstone removal with snare. c) Endoscopic laser lithotripsy. d) Fragmented gallstone. e) Gallstone fragment removal with snare. f) Ulcer at duodenum from impacted gallstone after lithotripsy.
Disclosures: Christopher G Ortiz-Morales indicated no relevant financial relationships. Sofia Frau Rivera indicated no relevant financial relationships.
Christopher G Ortiz-Morales, MD1, Sofia I. Frau Rivera, MD2. P1452 -
Case Report: Endoscopic Treatment of Bouveret Syndrome in a Nonagenarian—Overcoming Age-Related Challenges, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")