University of Massachusetts Chan Medical School - Baystate Health Springfield, MA
Prakriti Ramamurthy, MBBS, MD1, Advaith N. Rao, MBBS2, Thanisha Santhosh, MBBS2, Pranav Ramamurthy, MBBS, MD3, Rahul Ravindra, MBBS, MD4, Shivalinga Shekar, MD, DrNB5, Raj Vigna. Venugopal, MBBS, DNB, DM5, Vinayak Bhat, 6, Tripti Kaur, MD5 1University of Massachusetts Chan Medical School - Baystate Health, Springfield, MA; 2M S Ramaiah Medical College, Bangalore, Karnataka, India; 3University of Massachusetts Chan Medical School-Baystate Medical Center, Springfield, MA; 4White River Medical Center, Batesville, AR; 5Manipal Hospital, Bangalore, Karnataka, India; 6Henry M. Gunn Senior High School, Palo Alto, CA Introduction: Amyloidosis is a rare disease characterised by the deposition of misfolded proteins in various organs of the body, usually with multisystemic involvement. Isolated hepatic amyloidosis is a rare subset usually presenting with hepatomegaly and mild transaminitis. We report a rare case of hepatic amyloidosis presenting as portal hypertension and ascites due to hepatic vein obstruction which was complicated by hepatic subcapsular hemorrhage.
Case Description/
Methods: A 55 year old male presented with abdominal distension, fever, weight loss and jaundice for 2 months. Laboratory testing revealed direct hyperbilirubinemia, deranged coagulation parameters and hyponatremia. Endoscopy showed presence of gastroesophageal varices. Abdominal computed tomography showed a poorly enhancing nodular liver with large ascites, extensive varices and attenuated right hepatic vein, poor opacification of middle and left hepatic vein and a patent portal vein. Doppler ultrasonography showed right hepatic vein ostial narrowing for which hepatic vein balloon angioplasty was done. Transjugular liver biopsy was suggestive of non-AA/non-AL amyloidosis.
Falling hemoglobin levels prompted repeat imaging which revealed active bleeding from the right liver capsule, which was treated with hepatic artery embolization and transfusion of packed red cells. The patient required a prolonged intensive care stay for hemorrhagic shock, metabolic acidosis and disseminated intravascular coagulation, with course further complicated by spontaneous bacterial peritonitis. Echocardiogram was not consistent with cardiac amyloidosis. Per his preference, the patient was discharged for further systemic amyloidosis workup in the outpatient setting after gradual clinical improvement. Discussion: Isolated hepatic amyloidosis is a rare condition which can have a wide clinical spectrum but is typically mild. Our patient presented with stigmata of portal hypertension due to hepatic vein obstruction which is caused by amyloid infiltration leading to endothelial thickening and damage triggering the coagulation cascade. Hepatic amyloidosis should be considered as a differential in hepatic venous obstruction, and may need interventional management beyond anticoagulation. The increased risk of hemorrhage and severe hemorrhagic shock post liver biopsy in these cases is also due to vascular infiltration leading to fragility. This emphasizes the need to balance the risks and benefits of liver biopsy, especially when amyloidosis is on the differential.
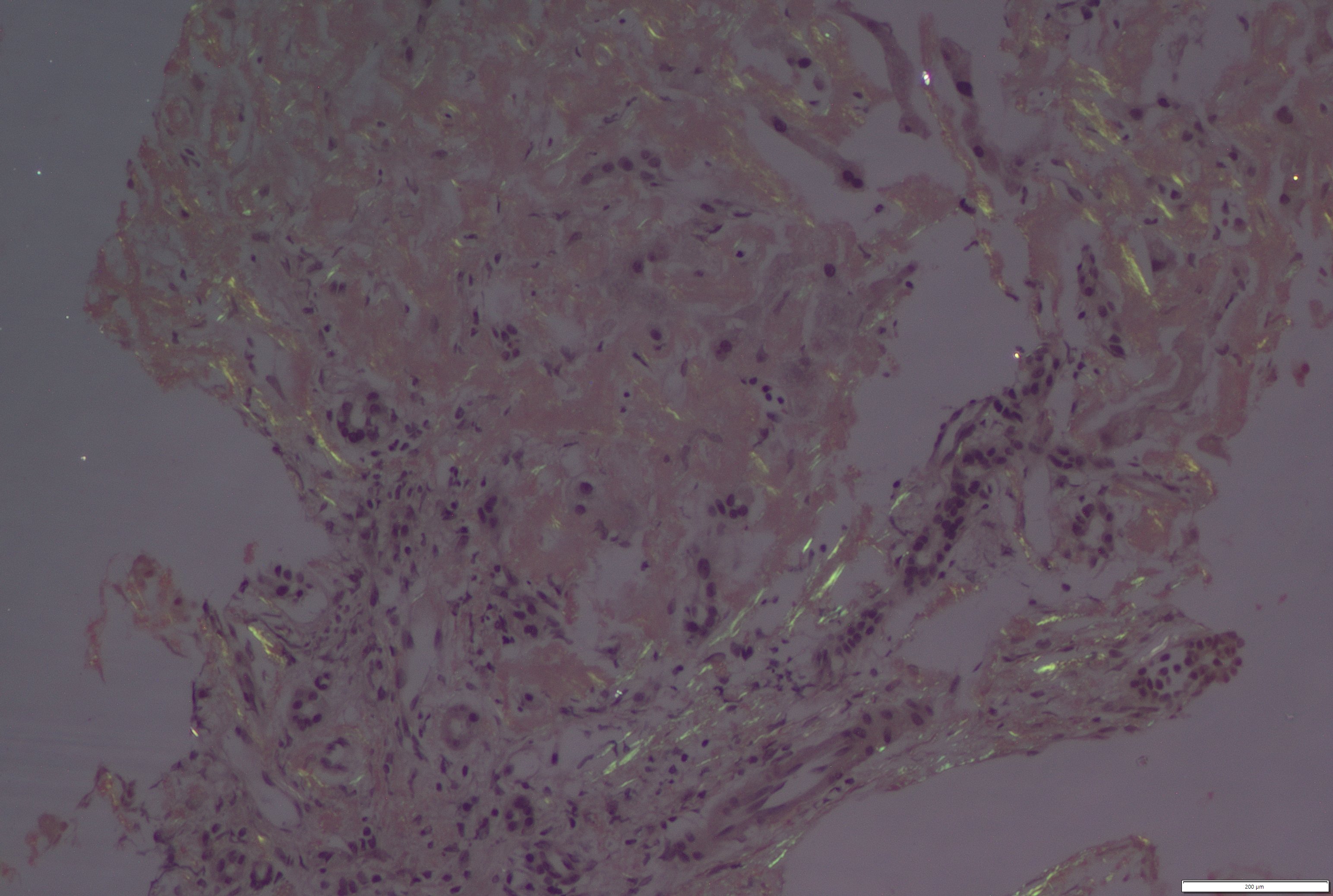
Figure: Congo red stain, 20x: Photomicrograph highlights amyloid deposits exhibiting apple green birefringence on polarising light.
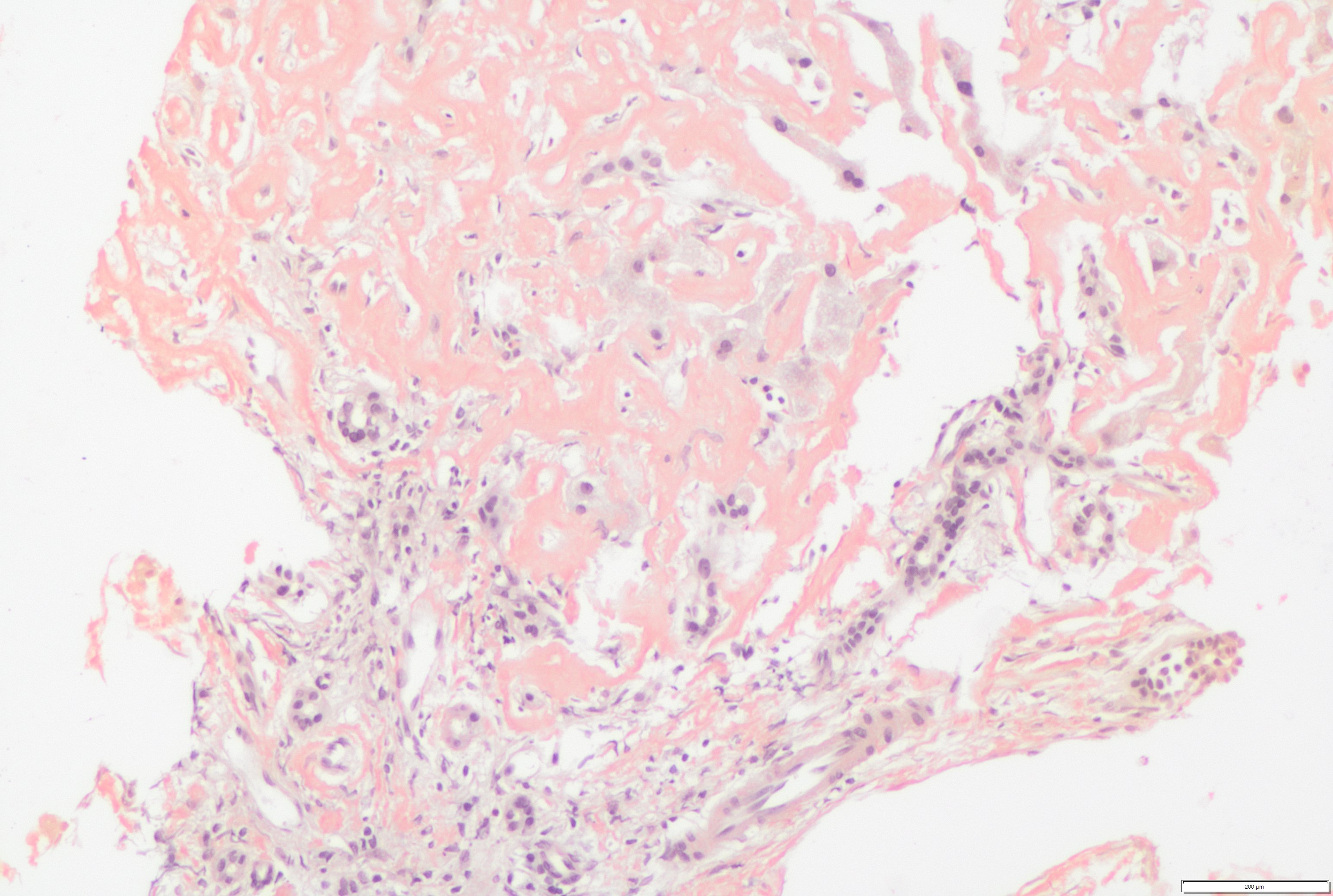
Figure: Congo red stain, 20x: Photomicrograph highlights amyloid deposits, which stain orange red (congophilic).
Disclosures: Prakriti Ramamurthy indicated no relevant financial relationships. Advaith Rao indicated no relevant financial relationships. Thanisha Santhosh indicated no relevant financial relationships. Pranav Ramamurthy indicated no relevant financial relationships. Rahul Ravindra indicated no relevant financial relationships. Shivalinga Shekar indicated no relevant financial relationships. Raj Venugopal indicated no relevant financial relationships. Vinayak Bhat indicated no relevant financial relationships. Tripti Kaur indicated no relevant financial relationships.
Prakriti Ramamurthy, MBBS, MD1, Advaith N. Rao, MBBS2, Thanisha Santhosh, MBBS2, Pranav Ramamurthy, MBBS, MD3, Rahul Ravindra, MBBS, MD4, Shivalinga Shekar, MD, DrNB5, Raj Vigna. Venugopal, MBBS, DNB, DM5, Vinayak Bhat, 6, Tripti Kaur, MD5. P1795 - Hepatic Vein Obstruction: An Atypical Presentation of Isolated Hepatic Amyloidosis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")