University of Rochester Medical Center Rochester, NY
Anuroop Yekula, MD1, Smriti Kochhar, DO2, Junseo Lee, MD1, Daniel Oppenheimer, MD1, Truptesh H. Kothari, MD, MS, FACG1 1University of Rochester Medical Center, Rochester, NY; 2Penn State Health Milton S. Hershey Medical Center, Hershey, PA Introduction: Emphysematous hepatitis (EH) is a rare, life-threatening necrotizing infection of the liver characterized by the presence of gas within the hepatic tissue, without a fluid collection, and after exclusion of iatrogenic, vascular or biliary sources of gas. The diagnosis is often delayed due to non-specific presentation, rapid progression and high mortality rate. The incidence of EH is extremely rare, with only 18 cases reported in the literature
Case Description/
Methods: A 79-year-old male with a history of coronary artery disease and prediabetes, presented to the hospital with progressively worsening fatigue, myalgias, and subjective fevers, chills, and abdominal pain. He appeared ill, with jaundice and diffuse abdominal tenderness. He was afebrile, hemodynamically stable. Initial electrocardiogram (EKG) showed sinus rhythm. He had significant leukocytosis to 22700/μL, normal platelets and INR. Total indirect bilirubin were 12.9 mg/dL and 9.7 mg/dL, respectively, AST 128 U/L and ALT 95 U/L.
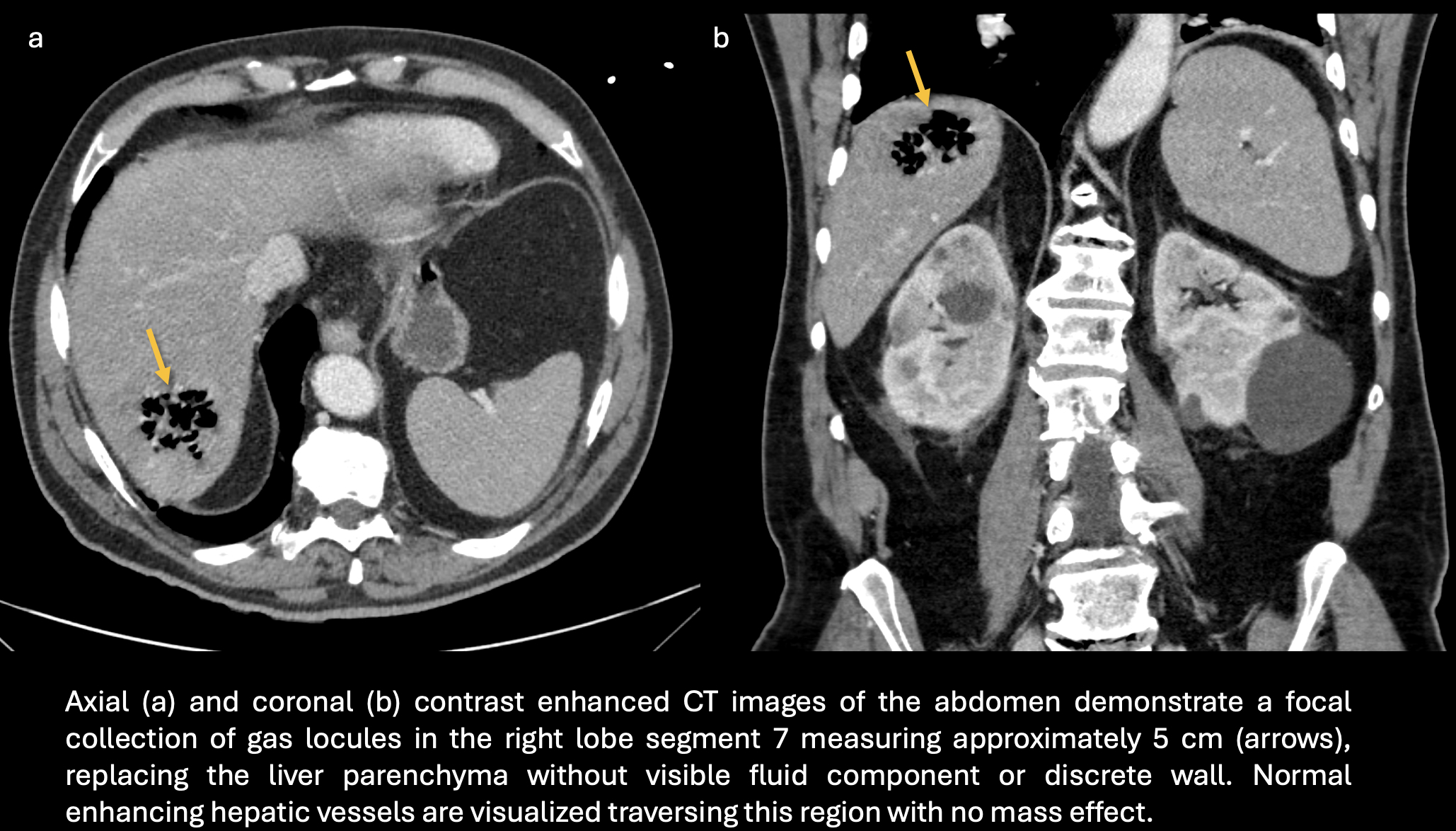
CT abdomen showed a focal collection of gas replacing liver parenchyma in the right hepatic lobe segment 7, approximately 5 cm, without any fluid components, vascular gas, or pneumobilia. Blood cultures were sent, and he was started on broad spectrum antibiotics. Unfortunately, over the next few hours, he had worsening hemodynamic status with new atrial fibrillation, hypotension requiring vasopressors. Despite appropriate resuscitation and critical care, he eventually succumbed to PEA cardiac arrest from ongoing fulminant sepsis.
The initial set of blood cultures eventually were positive for Clostridium perfringens, confirming the presence of gas-forming organisms. This case was discussed with the multidisciplinary team including diagnostic radiologist who confirmed the presentation and imaging findings were consistent with EH Discussion: EH is a rare and lethal infection of liver parenchyma caused by bacterial fermentation of necrotic tissue and the production of gases with rapid clinical progression to septic shock and organ failure. Diabetes mellitus is a common comorbidity in patients with EH. The initial management of EH involves aggressive resuscitation and broad-spectrum antibiotics. interventional or surgical drainage of the gas in the liver has been reported with some favorable results. Our case illustrates the rapidity of EH progression as the patient succumbed within hours after presentation to the emergency department, despite prompt imaging diagnosis and initiation of antimicrobial therapy
Figure: Emphysematous Hepatitis: CT Imaging
Disclosures: Anuroop Yekula indicated no relevant financial relationships. Smriti Kochhar indicated no relevant financial relationships. Junseo Lee indicated no relevant financial relationships. Daniel Oppenheimer indicated no relevant financial relationships. Truptesh Kothari indicated no relevant financial relationships.
Anuroop Yekula, MD1, Smriti Kochhar, DO2, Junseo Lee, MD1, Daniel Oppenheimer, MD1, Truptesh H. Kothari, MD, MS, FACG1. P1780 - Air Is the Enemy: A Fatal Case of Emphysematous Hepatitis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.