Ethan Shamsian, DO1, Joshua E. Pagán-Busigó, MD2, Raphael Shankman, BS1, Sameer Rao, MBBS1, Kranthi Mandava, MD1, Rohan Karkra, MBBS1, Berk Madendere, MD1, Mohammad-Ali Mousavi, DO3, Nina Brogle, MD4, Sima Vossough-Teehan, MD5 1Rutgers New Jersey Medical School, Newark, NJ; 2Rutgers New Jersey Medical School, Kearny, NJ; 3Department of Veterans Affairs-East Orange, East Orange, NJ; 4Rutgers New Jersey Medical School, East Orange, NJ; 5East Orange VA Hospital, East Orange, NJ Introduction: Azygous continuation of the inferior vena cava (ACIVC) is a rare congenital anomaly characterized by the absence of the intrahepatic IVC above the renal vasculature. Often associated with other congenital malformations, it is typically found incidentally in asymptomatic patients via contrast-enhanced CT or MRI. Misdiagnosis can occur due to azygous and hemiazygous vein enlargement mimicking other abnormalities. While ACIVC has been mistaken for various conditions, no reports exist of misdiagnosis as hepatic pathology. Here, we present a case of ACIVC mischaracterized as portal hypertension, mediastinal varices, and potential cirrhosis in a healthy 37-year-old male.
Case Description/
Methods: A 37-year-old male with arthralgia, lower back pain, and prior umbilical hernia repair presented with right groin pain and intermittent chest pain. Vitals, labs, and cardiac work-up were unremarkable. CT imaging ruled out an inguinal hernia but revealed left hepatic and caudate lobe enlargement, portal and azygous vein prominence, and large mediastinal and paraspinal varices. Initially assessed for cirrhosis, extensive liver workup was negative. A multidisciplinary review with radiology and vascular surgery determined the venous findings were due to ACIVC with collateral venous networks rather than cirrhosis. A follow-up CT angiogram confirmed IVC atresia with azygous engorgement. The patient's groin pain has since resolved, and vascular surgery deemed his chest pain to likely be musculoskeletal in origin. Discussion: This report highlights the diagnostic challenges of ACIVC, an often asymptomatic condition that can mimic serious pathologies, leading to misdiagnosis and unnecessary interventions.
IVC malformations are linked to complications such as DVT, pulmonary embolism, and asplenia-polysplenia syndromes. ACIVC has been misinterpreted as mediastinal masses, lung neoplasms, or aortic dissection. Our case is the first reported misdiagnosis of ACIVC as cirrhosis despite an unremarkable liver workup. In our patient, enlarged azygos and mediastinal veins were mistaken for varices suggesting cirrhosis, highlighting the need for comprehensive clinical, lab, and imaging correlation.
This case underscores the importance of recognizing ACIVC to prevent incorrect diagnoses, excessive treatments and improve patient outcomes. Collaboration between clinicians and radiologists is essential, and further research should focus on diagnostic algorithms and long-term management strategies.
Figure: CTA abdomen and pelvis revealing atresia of the IVC at the level of portohepatous (blue arrow)
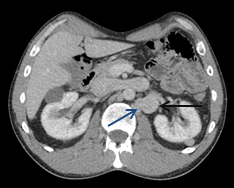
Figure: CTA abdomen and pelvis showing left vertebral collateral (blue arrow) and engorged left renal vein (black arrow)
Disclosures: Ethan Shamsian indicated no relevant financial relationships. Joshua Pagán-Busigó indicated no relevant financial relationships. Raphael Shankman indicated no relevant financial relationships. Sameer Rao indicated no relevant financial relationships. Kranthi Mandava indicated no relevant financial relationships. Rohan Karkra indicated no relevant financial relationships. Berk Madendere indicated no relevant financial relationships. Mohammad-Ali Mousavi indicated no relevant financial relationships. Nina Brogle indicated no relevant financial relationships. Sima Vossough-Teehan indicated no relevant financial relationships.
Ethan Shamsian, DO1, Joshua E. Pagán-Busigó, MD2, Raphael Shankman, BS1, Sameer Rao, MBBS1, Kranthi Mandava, MD1, Rohan Karkra, MBBS1, Berk Madendere, MD1, Mohammad-Ali Mousavi, DO3, Nina Brogle, MD4, Sima Vossough-Teehan, MD5. P1852 - Azygous Continuation of the IVC: Potential Misdiagnosis as Liver Cirrhosis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.