University of Arizona College of Medicine, Phoenix VA Medical Center Phoenix, AZ
Kelli Kosako Yost, MD1, Amy Jencks, DO2, Teodor C. Pitea, MD3, Hugo L.. Pinillos, MD, FACG4 1University of Arizona College of Medicine, Phoenix VA Medical Center, Phoenix, AZ; 2HonorHealth, Scottsdale, AZ; 3interventional Endoscopy Associates, Phoenix, AZ; 4Phoenix VA Health Care System, Phoenix, AZ Introduction: Bleeding originating from the small intestine makes up less than 10% of all cases of gastrointestinal bleeding and is typically from a vascular origin. Angiodysplasia is the most commonly implicated, but rarely other vascular lesions can be the culprit. We present a case of a benign vascular proliferation presenting as a small bowel mass causing recurrent gastrointestinal bleeding.
Case Description/
Methods: The patient is a 63 y.o male with PMH of T2DM, HTN, OSA, and HLD who presented with asymptomatic iron-deficiency anemia and a positive FIT test. Labs revealed a microcytic anemia with hemoglobin 8.5 g/dL (previously 12.5 g/dL one year prior), iron 23 mcg/dL, iron saturation 6%, transferrin 301 mg/dL, and ferritin 8 ng/dL. EGD was performed, which showed a few diminutive polyps in the gastric fundus and body, bulbar erythema, and lymphangiectasia in the 2nd portion of the duodenum. The biopsies showed mild chronic gastritis (H. pylori negative) and fundic gland polyps. Colonoscopy was completed showing small internal hemorrhoids and single medium sized cecal diverticulum. Capsule endoscopy was then pursued, revealing a large actively bleeding polypoid lesion with stalk, likely in the proximal/mid ileum. The patient was referred to an advanced endoscopist for double ballon enteroscopy and underwent piecemeal excision of the lesion with hot snare. The pathology of the lesion showed large feeder vessels in the submucosa and expansile proliferation of capillary vessels with no worrisome atypia. The biopsy was negative for amyloid, cytokeratin AE1/AE3, S100, CD117, desmin, ALK1, SMA, and HHV8, but positive for CD31 and CD34. Multiple pathologists confirmed the biopsies were consistent with a benign vascular proliferation that did not fit well into the pre-existing categories of AVM, Dieulafoy lesions, or lobular capillary hemangioma. Discussion: The most common causes of small intestine bleeding in older adults are angiodysplasias, Dieulafoy’s lesions, neoplasia, and NSAID-induced ulcers. Mass-like lesions seen on endoscopic evaluation are worrisome for underlying neoplasm. This case highlights a unique etiology of small bowel bleeding: benign vascular proliferation presenting as a “pseudoneoplasm.” Vascular pseudoneoplasms of the small intestine are exceedingly rare and can lead to bowel intussusception and recurrent bleeding, as seen in this patient. This case also highlights the importance of video capsule endoscopy for detecting uncommon causes of small intestinal bleeding.
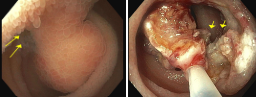
Figure: Lesion on double balloon enteroscopy
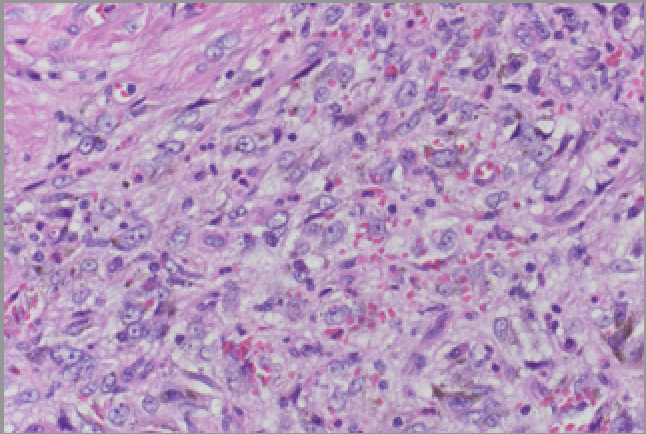
Figure: Histology with H&E staining at 40x magnification
Disclosures: Kelli Kosako Yost indicated no relevant financial relationships. Amy Jencks indicated no relevant financial relationships. Teodor Pitea: Olympus – Consultant. Hugo Pinillos indicated no relevant financial relationships.
Kelli Kosako Yost, MD1, Amy Jencks, DO2, Teodor C. Pitea, MD3, Hugo L.. Pinillos, MD, FACG4. P1954 - Benign Vascular Proliferation of the Small Intestine Presenting as a Pseudoneoplasm, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.