Abby Kunitsky, DO1, Mario Hanna, BS2, Julia Janecki, DO1, Tariq Hassan, DO1, Jaspreet Ghumman, DO1 1McLaren Macomb, Mt. Clemens, MI; 2Michigan State University College of Osteopathic Medicine, East Lansing, MI Introduction: Mesothelioma is a rare, aggressive malignancy of mesothelial cells, typically affecting the pleura and, less commonly, the peritoneum. Primary omental mesothelioma is exceedingly rare, with limited reported cases. Unlike pleural or peritoneal forms, omental mesothelioma is less often associated with asbestos exposure. Clinical symptoms are usually vague, such as nonspecific abdominal pain or distension, complicating timely diagnosis. Imaging can mimic metastatic or inflammatory diseases, requiring histopathological confirmation with immunohistochemistry (IHC) for diagnosis.
Case Description/
Methods: An 81-year-old female with gastroesophageal reflux disease presented with over a year of intermittent, right-sided abdominal pain lasting 15–30 minutes, unrelated to meals, bowel movements, or activity. She had no known asbestos exposure. Workup later revealed an elevated chromogranin A (1883 ng/mL) and serotonin (250 ng/mL), attributed in part to proton pump inhibitor use. Despite conservative management, her pain persisted. Serial imaging demonstrated evolving omental and mesenteric abnormalities—fat stranding, ascites, a peritoneal enhancement, and retroperitoneal lymphadenopathy. Multiple paracenteses were nondiagnostic; cytology remained negative for malignancy, although ascitic fluid had a low serum-ascites albumin gradient. Due to the radiographic progression of thickened nodular omentum, a CT-guided omental biopsy was able to be performed. Histology confirmed malignant mesothelioma with positive staining for calretinin, Wilms tumor-1 antigen (WT-1), cytokeratin (CK) 5/6, podoplanin (D2-40), and cytokeratin 7. The patient elected for conservative management and palliative chemotherapy. Discussion: Primary omental mesothelioma remains a diagnostic challenge due to its rarity and nonspecific presentation. Imaging may mimic other abdominal pathologies, while cytologic analysis of ascitic fluid can be falsely negative. This case highlights the importance of maintaining suspicion for malignancy in the setting of persistent symptoms and abnormal findings. Tissue biopsy and IHC is a crucial diagnostic element when less invasive tests are inconclusive, but do require a large enough sample to biopsy. Typical expression of mesothelial markers include calretinin, WT-1, CK5/6, D2-40, and mesothelin. No standardized treatment guidelines exist, and prognosis is poor. Gastroenterologists play a pivotal role in identifying atypical malignancies and facilitating timely diagnosis and care.
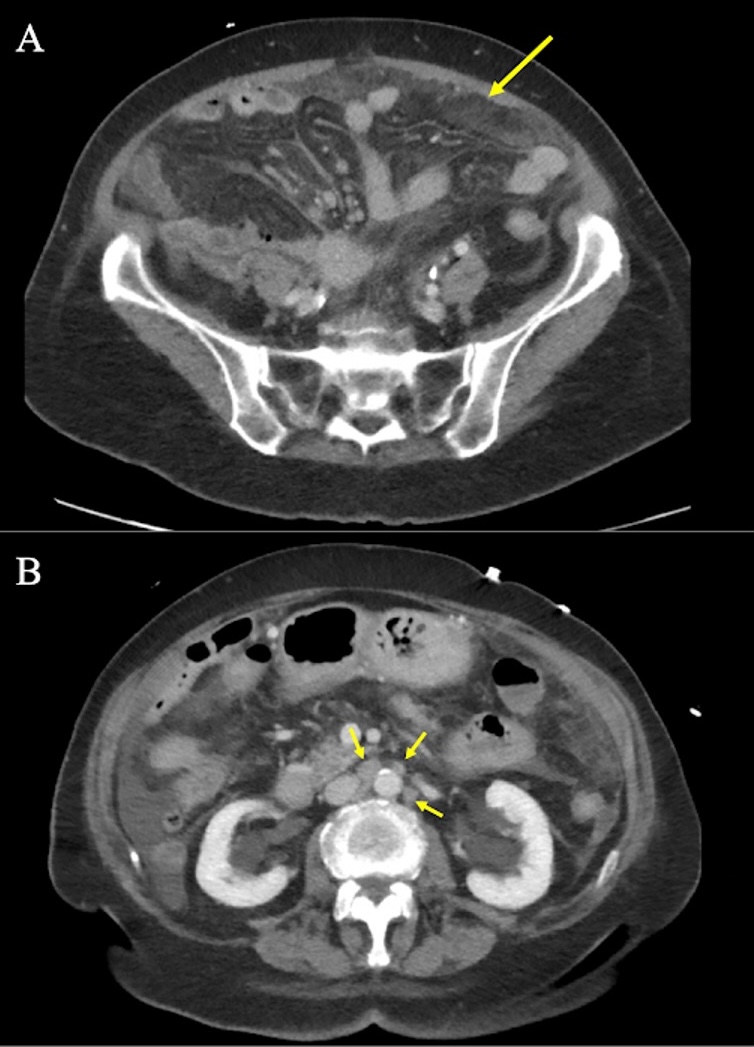
Figure: Figure 1: CT of the abdomen and pelvis with contrast demonstrating A) thickened nodular omentum (yellow arrow) and B) retroperitoneal lymphadenopathy (yellow arrows).
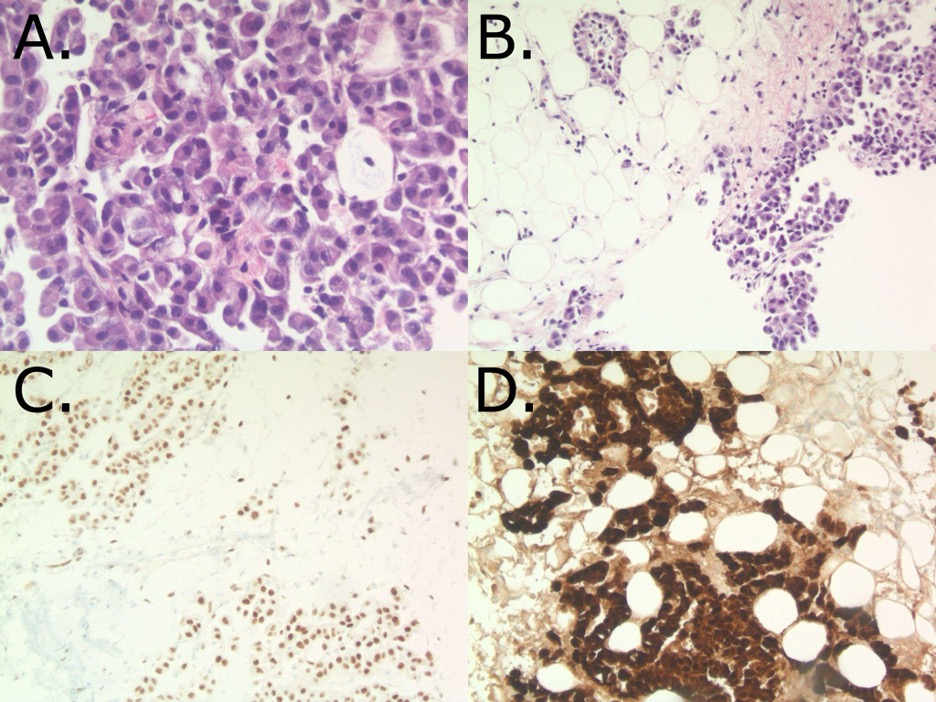
Figure: Figure 2: A & B) H&E staining of omental tissue demonstrating epithelioid pleomorphic tumor cells with eccentric nuclei. Tumor cells were diffusely positive for tumor markers WT1 (C) and Calretinin (D) on immunostain (brown fluorescence).
Disclosures: Abby Kunitsky indicated no relevant financial relationships. Mario Hanna indicated no relevant financial relationships. Julia Janecki indicated no relevant financial relationships. Tariq Hassan indicated no relevant financial relationships. Jaspreet Ghumman indicated no relevant financial relationships.
Abby Kunitsky, DO1, Mario Hanna, BS2, Julia Janecki, DO1, Tariq Hassan, DO1, Jaspreet Ghumman, DO1. P1951 - Primary Omental Mesothelioma: A Case-Based Perspective Highlighting Diagnostic Challenges, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.