Maniel A. Ruiz-Ramos, MD, Belissa Lopez-Peña, MD, Brian D. Virella-Berio, MD San Juan City Hospital, San Juan, Puerto Rico Introduction: Follicular lymphoma (FL) is the most common indolent non-Hodgkin lymphoma, but its presence in the gastrointestinal (GI) tract is rare, accounting for only 1–8% of GI malignancies. Among these, the duodenum is the most frequently affected site, representing up to 89% of GI FL cases. Despite increasing recognition, primary duodenal follicular lymphoma (DFL) remains uncommon, and there are no specific guidelines for its diagnosis or management. Clinical evaluation often mirrors that of nodal FL, relying on histologic confirmation, imaging, and risk stratification using the Follicular Lymphoma International Prognostic Index (FLIPI).
Case Description/
Methods: A 50-year-old Hispanic male with hypertension presented with diffuse abdominal pain, early satiety, poor oral intake, and multiple episodes of non-bloody emesis. Denied weight loss, fever, or chills. CT imaging revealed circumferential thickening of a 9.5 cm segment of the distal duodenum and associated mesenteric lymphadenopathy. Upper endoscopy showed mucosal erythema, erosions, and inflammation in the third portion of the duodenum, initially raising concern for peptic ulcer disease. Biopsies revealed duodenal-type FL, confirmed by immunohistochemistry: CD20+, CD21+, CD23+, BCL2+, and weak BCL6+. One month later, the patient returned with worsening abdominal pain and emesis. Repeat imaging showed a progressive duodenal mass causing small bowel obstruction. He underwent exploratory laparotomy with gastrojejunal anastomosis (Billroth II) and placement of a feeding jejunostomy. This case illustrates a rare complication of DFL, mechanical obstruction despite its typically indolent nature. Discussion: Endoscopically, DFL often appears as small, whitish polypoid nodules or subepithelial lesions. While it usually follows a slow, favorable clinical course with minimal risk of transformation, this case highlights that complications like obstruction may occur. Given its rarity and nonspecific presentation, DFL should remain a diagnostic consideration in cases of unexplained duodenal thickening or mucosal abnormalities, especially when other causes (e.g., H. pylori) are ruled out. Diagnosis should include biopsy, immunophenotyping, full-body imaging, and bone marrow evaluation. Early identification is essential to guide appropriate therapy and prevent serious outcomes.
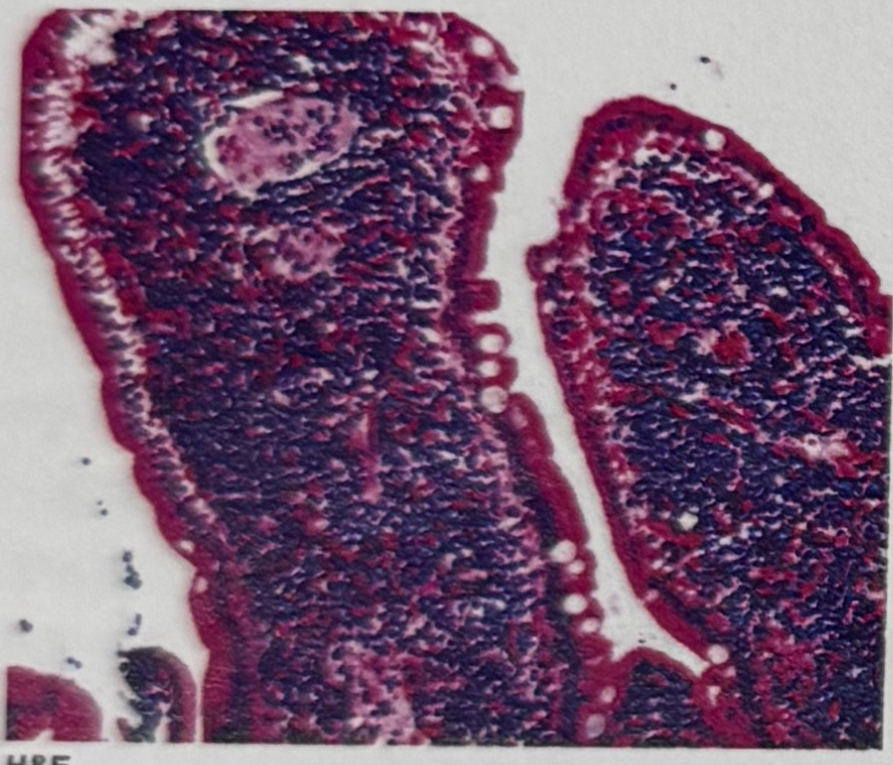
Figure: Duodenum biopsy remarkable for duodenal type follicular lymphoma
Figure: Endoscopic image of the third portion of duodenum with erosions and erythema with friable mucosa with discrete area of mucosal inflammation
Disclosures: Maniel Ruiz-Ramos indicated no relevant financial relationships. Belissa Lopez-Peña indicated no relevant financial relationships. Brian Virella-Berio indicated no relevant financial relationships.
Maniel A. Ruiz-Ramos, MD, Belissa Lopez-Peña, MD, Brian D. Virella-Berio, MD. P1942 - From Subtle GI Symptoms to Surgical Abdomen: An Unusual Presentation of Duodenal Follicular Lymphoma, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")