Columbia University Irving Medical Center New York, NY
Award: ACG Presidential Poster Award
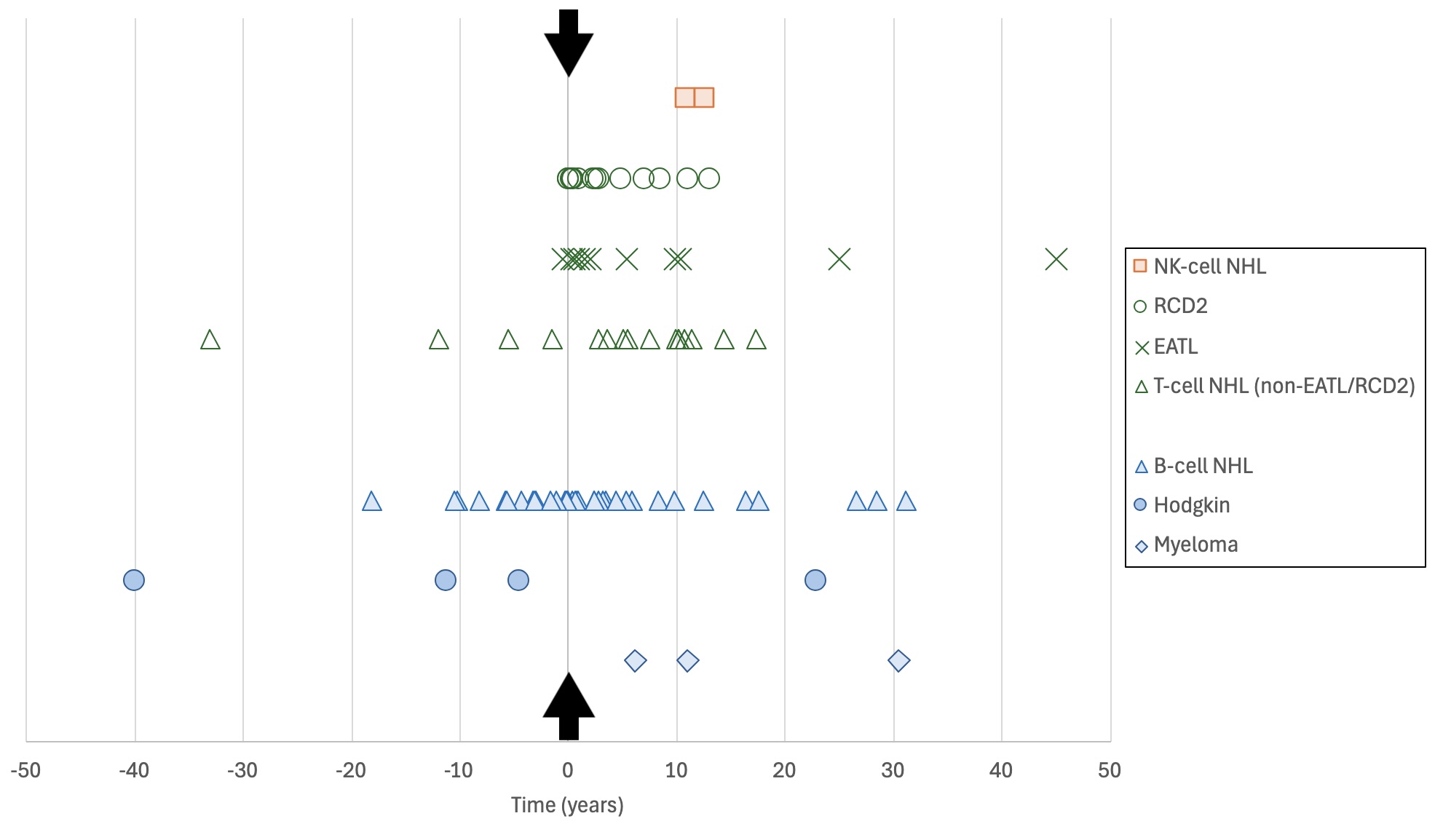
David R. Veal, MD, John B. Doyle, MD, Suzanne K. Lewis, MD, Govind Bhagat, MD, Peter H. Green, MD, Benjamin Lebwohl, MD, MS Columbia University Irving Medical Center, New York, NY Introduction: Celiac disease (CeD) is associated with an increased risk of enteropathy-associated T-cell lymphoma (EATL) and other non-Hodgkin lymphomas (NHL), which contribute to increased mortality risk. In the general population, cases of B-cell NHL far outnumber T-cell NHL. Our aim was to compare CeD patients diagnosed with a lymphoproliferative disorder (LPD) before CeD diagnosis to those diagnosed with an LPD concurrently or after CeD diagnosis. Methods: We performed a retrospective study of adult patients seen at our tertiary referral center between 1980 and 2024. Diagnosis of CeD was confirmed by villous atrophy on duodenal biopsy and/or by positive CeD serology. LPD was defined as a lymphoid malignancy, including multiple myeloma, Hodgkin lymphoma, NHL, and refractory celiac disease type II, considered to be a precursor of EATL. Diagnosis of CeD and LPD within one year was considered concurrent. Results: There were 87 cases of LPD identified in 82 patients, with four patients developing more than one LPD. There were 41 cases of T-cell NHL, with 90% presenting concurrently or after CeD diagnosis. The four cases presenting before CeD diagnosis were cutaneous: cutaneous anaplastic lymphoma kinase-negative anaplastic large cell lymphoma, cutaneous T-cell lymphoma (two cases), and lymphomatoid papulosis type A. There were 36 cases of B-cell NHL, with 31% presenting before and 69% presenting concurrently or after CeD diagnosis.
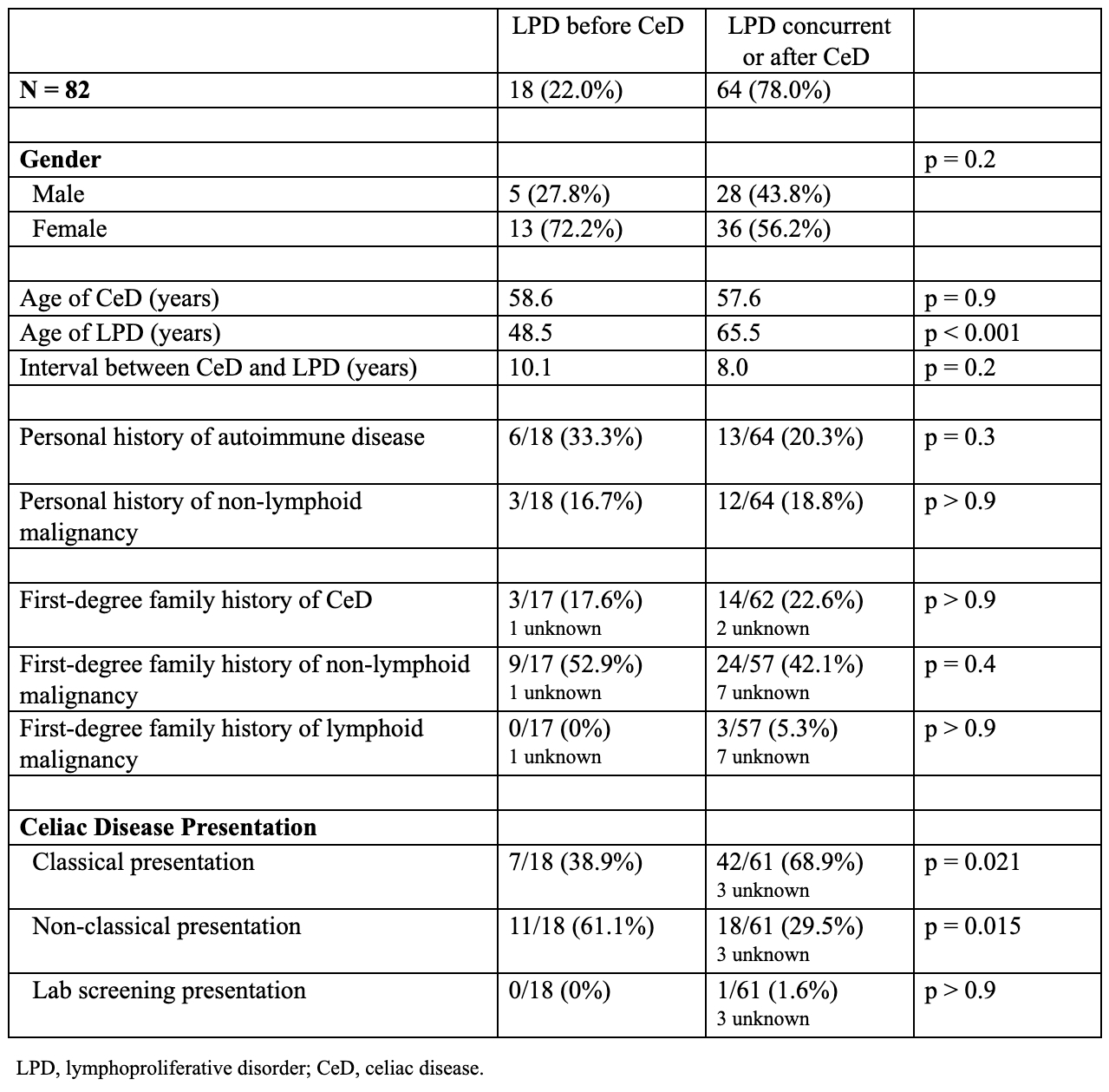
Comparing patients diagnosed with LPD before CeD diagnosis to those diagnosed concurrently or after CeD diagnosis, we found a mean age of CeD diagnosis of 58.6 and 57.6 years (p = 0.9), respectively, and a mean age of LPD diagnosis of 48.5 and 65.5 years (p < 0.001), respectively. Classical CeD presentation was seen in 38.9% and 68.9% of patients (p = 0.021), respectively. After LPD diagnosis, the median survival of patients with B-cell NHL was longer than for those with T/NK-cell NHL (18.6 versus 9.4 years, p = 0.008). Discussion: In this series, both B-cell and T-cell NHL cases were seen in CeD patients. Patients with B-cell NHL had longer median survival than those with T/NK-cell NHL. Patients diagnosed with LPD concurrently or after CeD diagnosis were more likely to have had a classical CeD presentation. Cases of T-cell NHL presenting before CeD diagnosis consisted of a small, heterogeneous group of cutaneous lymphomas, while the vast majority of T-cell NHLs were diagnosed concurrently or after CeD diagnosis.
Figure: Figure 1. Timing of LPD diagnosis relative to CeD diagnosis. The x-axis represents time, with the arrows indicating time of CeD diagnosis, or x = 0. The y-axis represents different categories of LPD. LPD, lymphoproliferative disorder; NK, natural killer; NHL, non-Hodgkin lymphoma; RCD2, refractory celiac disease type II; EATL, enteropathy-associated T-cell lymphoma.
Figure: Table 1. Characteristics of patients diagnosed with CeD and LPD
Disclosures: David Veal indicated no relevant financial relationships. John Doyle indicated no relevant financial relationships. Suzanne Lewis indicated no relevant financial relationships. Govind Bhagat: Blueprint Medicines – Non-branded educational talks. Peter Green indicated no relevant financial relationships. Benjamin Lebwohl indicated no relevant financial relationships.
David R. Veal, MD, John B. Doyle, MD, Suzanne K. Lewis, MD, Govind Bhagat, MD, Peter H. Green, MD, Benjamin Lebwohl, MD, MS. P1935 - Timing of Lymphoproliferative Disorder Diagnosis in Patients With Celiac Disease, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.