Kirk Kerkorian School of Medicine at the University of Nevada Las Vegas Las Vegas, NV
Magnus Chun, MD, Yassin Naga, MD, Jose Aponte-Pieras, MD Kirk Kerkorian School of Medicine at the University of Nevada Las Vegas, Las Vegas, NV Introduction: Gastrointestinal (GI) non-Hodgkin’s lymphoma (NHL) most often occurs due to widespread nodal disease with Diffuse Large B-cell lymphoma (DLBCL) being the most common subtype.1 However, primary GI NHL is rare, comprising of 1-4% of all GI neoplasms.2 Even more rare is primary GI NHL arising from multiple sites within the GI tract.3 We present a rare case of a patient with primary DLBCL of both the antrum and duodenum.
Case Description/
Methods: A 55-year-old male with a past medical history of HIV/AIDS (CD4 83 cells/mm3, viral load 25250 copies/mL) and syphilis presented with generalized weakness, diffuse abdominal pain unrelated to oral intake, and peripheral lower extremity edema for the past few months. He endorsed having significant unintentional weight loss. Clinical examination revealed abdominal tenderness to palpation diffusely. Pertinent labs included hemoglobin of 6.9 g/dL (MCV 87.6), alkaline phosphatase of 472 IU/L, ALT of 16 IU/L, and AST of 35 IU/L. Both CMV and EBV viral load were elevated at 7796 copies/mL and 18200 copies/mL, respectively. CT angiogram of the abdomen revealed an enlarged gastric lymph node measuring 13 mm and irregular gastric thickening of the lesser curvature. Upper endoscopy revealed a giant ulcerated mass extending from the proximal body to the antrum with heaped up margins and an ulcerated necrotic base, in which biopsies were taken (Figure 1a). There were also multiple duodenal nodules with biopsies taken (Figure 1b). Pathology and immunohistochemistry of the gastric mass and duodenal nodules revealed primary DLBCL with positive CD10 cells and EBV (Figure 2). After goals of care discussion, the patient was referred to Oncology for further therapy. Discussion: The GI tract is the most common site for extranodal secondary lymphoma. However, primary GI DLBCLs are rare GI malignancies.2 Our patient had primary GI DLBCLs in 2 different locations which is rarely seen in clinical practice. Primary GI DLBCLs can be easily missed as it can present with nonspecific symptoms as seen in our patient. When suspected, biopsies should be taken endoscopically to confirm lymphoma in addition to molecular analysis to accurately diagnose the lymphoma subtype for treatment guidance.4 Treatment of GI DLBCLs requires a multidisciplinary team including a gastroenterologist, oncologist, and a surgeon. Complications, such as perforation of the bowel, are common during surgical treatment.
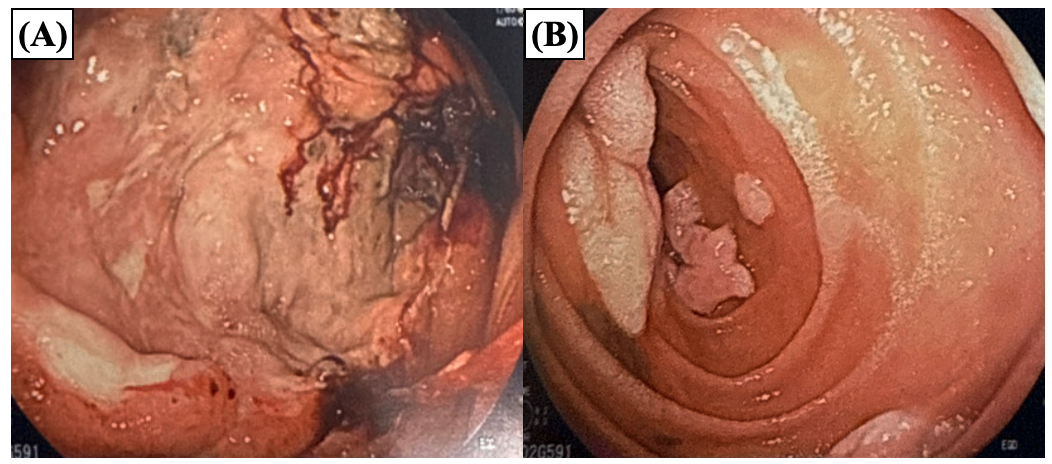
Figure: Figure 1. Upper endoscopy revealed a (A) giant ulcerated mass extending from the proximal body to the antrum with heaped up margins and an ulcerated necrotic base, in which biopsies were taken. (B) There were also multiple duodenal nodules with biopsies taken.
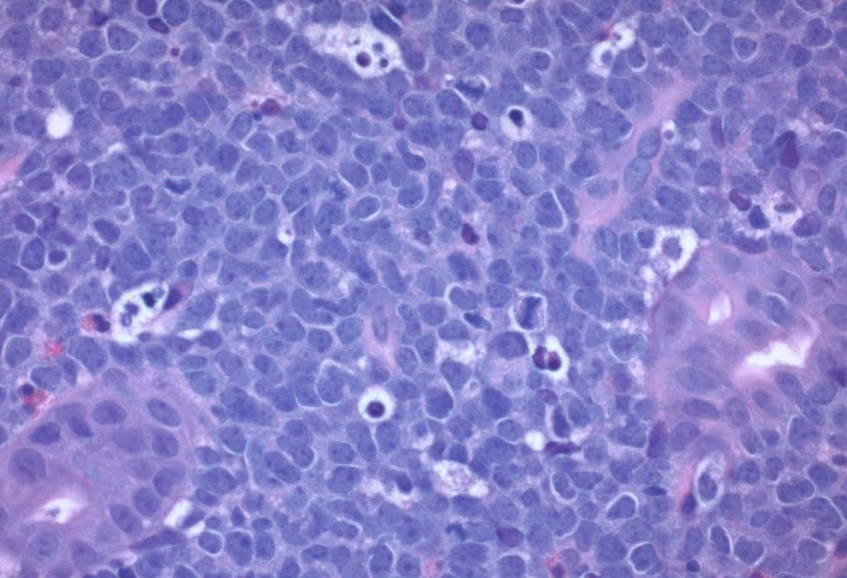
Figure: Figure 2. Pathology and immunohistochemistry of the gastric mass and duodenal nodules revealed primary DLBCL with positive CD10 cells and EBV.
Disclosures: Magnus Chun indicated no relevant financial relationships. Yassin Naga indicated no relevant financial relationships. Jose Aponte-Pieras indicated no relevant financial relationships.
Magnus Chun, MD, Yassin Naga, MD, Jose Aponte-Pieras, MD. P2018 - A Rare Case of Primary Gastrointestinal Diffuse Large B-Cell Lymphoma Arising From the Antrum and Duodenum, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.