Shruti Jain, MD1, Pooja Shah, MD2, Rohit Goyal, MD3, Karan Sachdeva, MD1, David Scott, MD4, Sudha Pandit, MD3 1LSU Health, Shreveport, LA; 2LSU Health Shreveport, Shreveport, LA; 3Louisiana State University, Shreveport, LA; 4LSU Health Sciences Center - SHREVEPORT, LA, Shreveport, LA Introduction: Gastric leiomyosarcomas are extremely rare tumors arising from the muscularis propria of the stomach. With the advent of immunohistochemistry, many tumors previously diagnosed as gastrointestinal stromal tumors (GIST) are now reclassified under leiomyosarcoma, making them account for less than 1% of all gastric tumors. In this case report, we present an unusual presentation of gastric leiomyosarcoma.
Case Description/
Methods: A 66-year-old female with a past medical history of congestive heart failure (CHF), atrial fibrillation on Eliquis, Pulmonary hypertension, and Chronic Obstructive Pulmonary disease (COPD). She presented to the emergency department with dyspnea on exertion and bilateral lower extremity edema and was admitted for the treatment of CHF exacerbation. Routine laboratory investigations revealed hypochromic microcytic anemia, with a hemoglobin level of 5.6 g/dL (baseline of 11.2 g/dL five months ago). A CT of the abdomen and pelvis with contrast did not reveal any significant abnormalities but was limited due to the patient's body habitus and a large abdominal hernia.
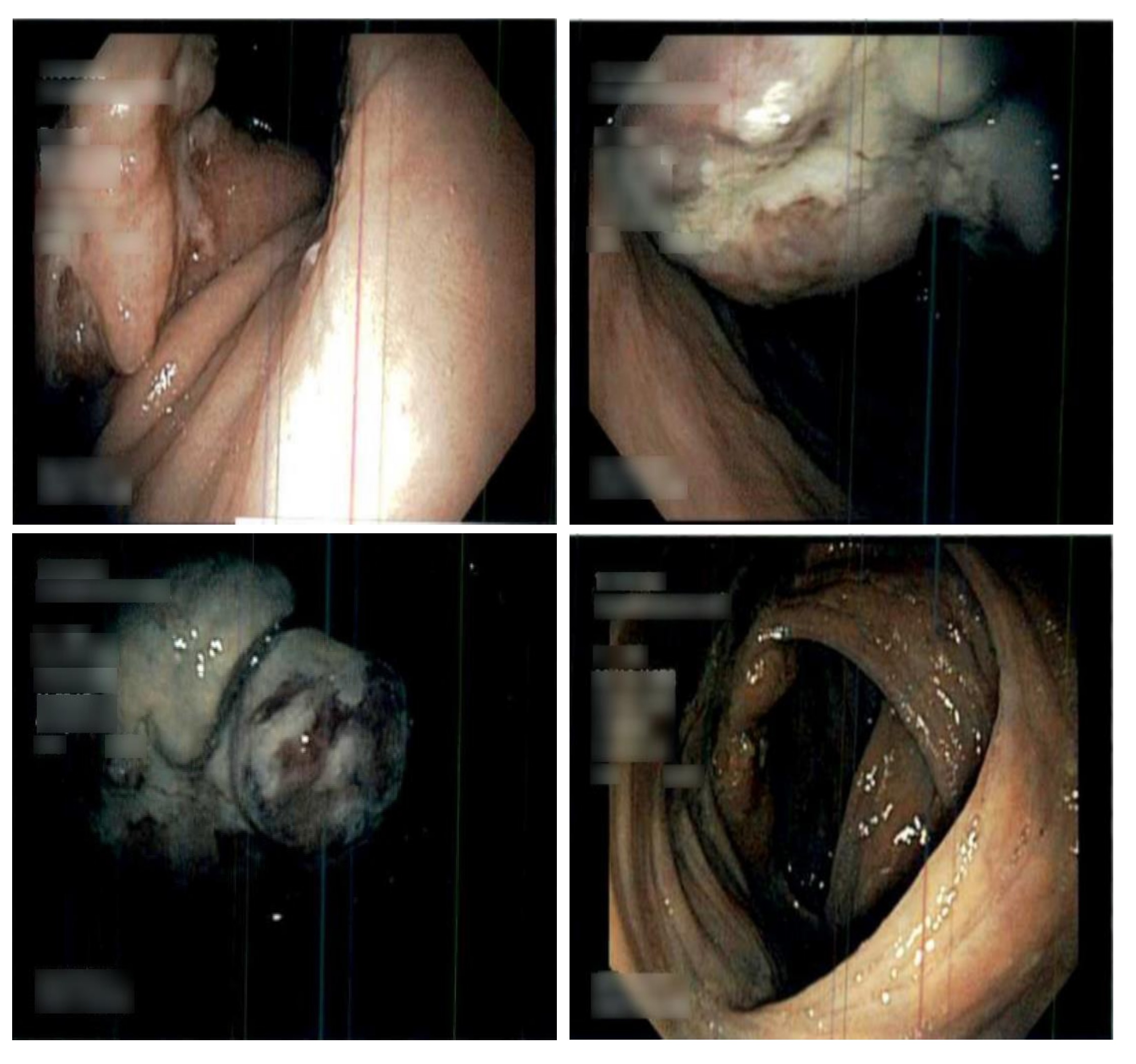
Esophagogastroduodenoscopy (EGD) revealed a large, ulcerated mass in the cardia of the stomach along with a large hiatal hernia. A biopsy of the mass confirmed the diagnosis of gastric leiomyosarcoma. Despite the patient’s elevated risk due to multiple comorbidities, overall risk-benefit analysis favors surgical intervention. Discussion: Our case highlights an incidental diagnosis of the tumor in a patient who initially presented with CHF exacerbation, possibly exacerbated by anemia secondary to chronic gastrointestinal bleeding from the tumor. The most common presentations of gastric leiomyosarcoma include nausea, vomiting, weight loss, upper gastrointestinal bleeding, and a palpable mass. Imaging and tissue diagnosis are crucial for accurate identification. CT imaging typically shows a large heterogeneous mass with peripheral solid enhancement and central areas of necrosis, hemorrhage, or degeneration. A tissue biopsy is required for definitive diagnosis.
Unfortunately, there is limited data on the benefits of chemotherapy and radiotherapy for gastric leiomyosarcoma. Surgical resection remains the standard of treatment. Further research into the potential benefits of chemotherapy and immunotherapy could benefit patients like ours, where surgical intervention carries significant risks due to cardiovascular comorbidities.
Figure: Figure 1: Gastric leiomyosarcoma as visualized on esophagogastroduodenoscopy (EGD): large ulcerated mass in cardia at 60 cm from incisors and 15 cm hiatal hernia.
Disclosures: Shruti Jain indicated no relevant financial relationships. Pooja Shah indicated no relevant financial relationships. Rohit Goyal indicated no relevant financial relationships. Karan Sachdeva indicated no relevant financial relationships. David Scott indicated no relevant financial relationships. Sudha Pandit: Medtronic – Product feedback.
Shruti Jain, MD1, Pooja Shah, MD2, Rohit Goyal, MD3, Karan Sachdeva, MD1, David Scott, MD4, Sudha Pandit, MD3. P2094 - Hidden in Plain Sight: An Incidental Discovery of Gastric Leiomyosarcoma, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")