Monday Poster Session
Category: Colon
Hussein Bazzy, DO
Corewell Health
Farmington Hills, MI
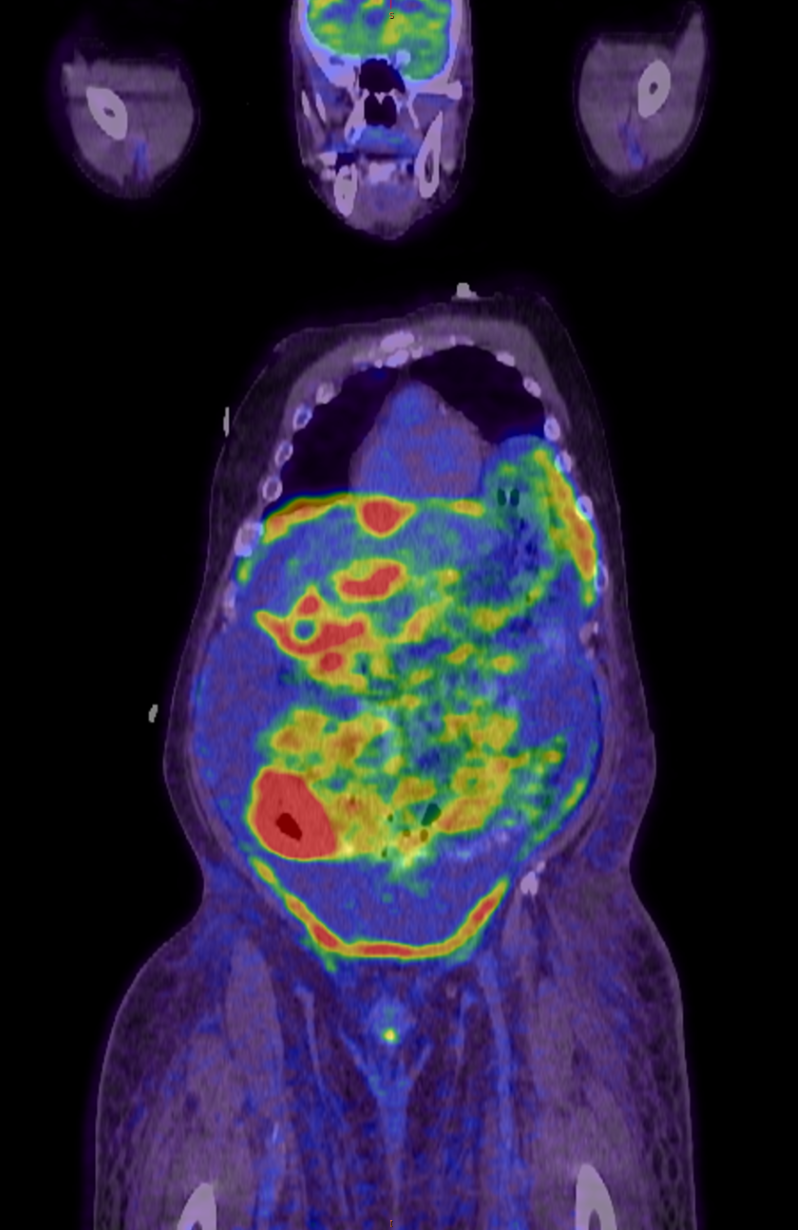
A 70-year-old African American male with a past medical history of Roux-en-Y gastric bypass who presented with poor appetite, abdominal distension, and reported 20 lbs. unintentional weight loss. On physical exam, abdomen was distended with mild, diffuse tenderness to palpation. Labs were notable for AST 157, ALT 106. Computed tomography of the abdomen and pelvis showed hepatocellular disease with subtle nodular liver contour with additional low attenuating lesions throughout the liver. He tested positive for Hepatitis B surface antigen with a viral load greater than 10^9 U/mL. Prior to this presentation, the patient had not been diagnosed with cirrhosis and denied regular alcohol consumption or unprotected sexual encounters.
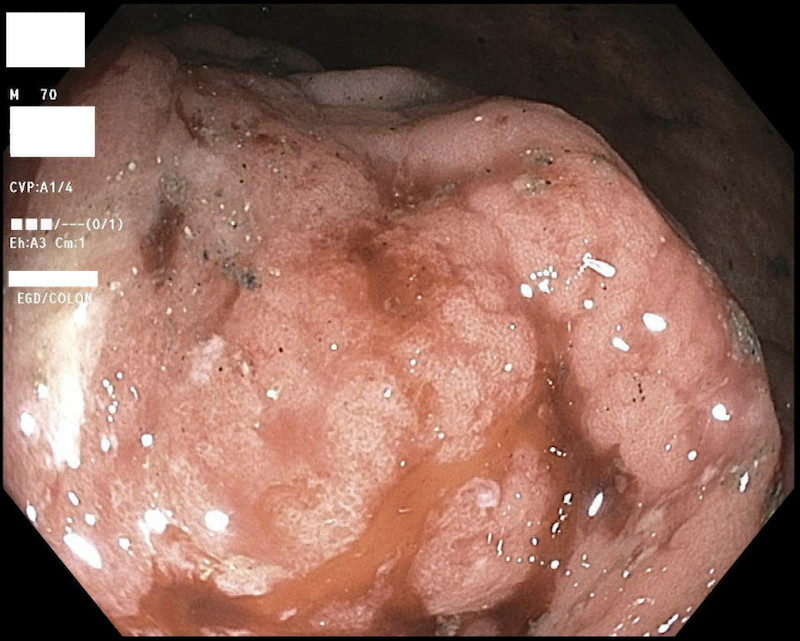
In the setting of numerous liver lesions, endoscopic evaluation was performed, with colonoscopy being notable for an ulcerated and friable cecal mass near the appendiceal orifice (Figure). Cecal biopsies were significant for aggressive/high-grade B cell lymphoma, germinal center type, by Hans algorithm. The lymphoma cells were positive for CD45, CD20, CD10, BCL 6, and MYC and Ki-67 of 100%.
The patient was started on dose-adjusted rituximab, etoposide, prednisone, vincristine, cyclophosphamide, and doxorubicin (DA-R-EPOCH) for management of aggressive B cell lymphoma with concern for possible Burkitt’s versus double hit lymphoma in the setting of Ki-67 of 100%. He was initiated on tenofovir for management of chronic hepatitis B, transitioned to entecavir shortly after due to renal dysfunction.