
Monday Poster Session
Category: Colon
 photo")
Faizan Ahmed, MD (he/him/his)
HCA Florida Healthcare
Clearwater, FL
Colorectal carcinoma remains a global burden despite screening gains¹. Metastases usually involve liver, lung, and distant nodes²; direct small-bowel invasion is rare and portends poor survival³. We describe a rectosigmoid adenocarcinoma perforating the jejunum, highlighting diagnostic clues and operative planning.
Case Description/
Methods:
A 66-year-old woman presented with palpitations. Vitals: heart rate 124, blood pressure 96/54mmHg. Labs: Hemoglobin 4.4g/dL, iron-deficiency indices. Digital rectal exam produced bright-red blood. After six units packed red blood cells, Esophagogastroduodenoscopy (EGD) was normal. Colonoscopy showed grade 4 hemorrhoids and a circumferential rectosigmoid mass > 15cm from anal verge; biopsy: moderately differentiated adenocarcinoma. Computed Tomography (CT) chest/abdomen/pelvis revealed a 9.4cm polypoid mass, eight enlarged regional nodes, and an 8mm posterior perirectal node. A ureteral stent safeguarded the left ureter. Open rectosigmoidectomy with en-bloc jejunal resection and diverting ileostomy was done after intra-operative perforation into adhered bowel. Post-op sepsis was managed with broad antibiotics. Pathology: T4bN1a stage IIIc adenocarcinoma (1/16 nodes). Adjuvant chemotherapy was planned.
Discussion:
About 70% of colorectal cancers are sporadic adenocarcinomas¹. Left-sided tumors present with obstruction and hematochezia; right-sided with occult bleeding and anemia². Small-bowel involvement occurs in < 2% of colorectal cancers and is usually metastatic³–⁵. Direct invasion defines T4b disease, mandates multivisceral en-bloc resection, and worsens prognosis⁶. Severe iron-deficiency anemia plus overt bleeding expedited colonoscopy, allowing diagnosis before complete obstruction. Imaging hinted at jejunal invasion, confirmed only during surgery. Curative therapy depends on radical resection with adequate nodal harvest; adjuvant chemotherapy improves stage III outcomes⁴. Surgeons should anticipate multivisceral resection and coordinate ureteral protection and multidisciplinary care in such advanced cases.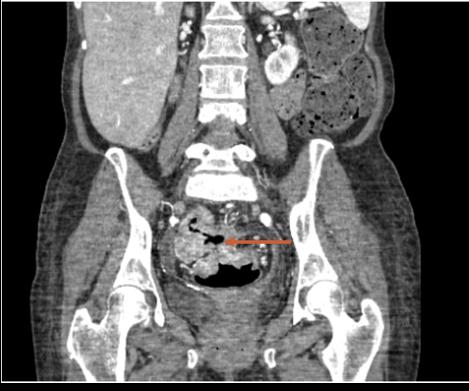
Figure: Figure 1. Computed tomography (CT) chest, abdomen and pelvis showed a polypoidal soft tissue mass involving the proximal rectum and rectosigmoid colon, with a segmental length of approximately 9.4 cm (orange arrow).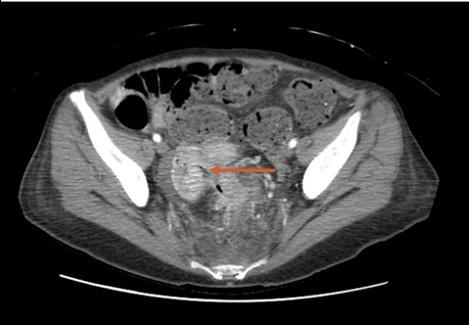
Figure: Figure 2. A right posterior perirectal lymph node was noted to be 8mm, as well as a total of 8 enlarged lymph nodes identified in this imaging study (orange arrow).
Disclosures:
Faizan Ahmed indicated no relevant financial relationships.
Andrew Ondracek indicated no relevant financial relationships.
Joshua Wais indicated no relevant financial relationships.
Joseph Armotrading indicated no relevant financial relationships.
Patrick Stocker indicated no relevant financial relationships.
Olugbenga Oyesanmi indicated no relevant financial relationships.
Faizan Ahmed, MD1, Andrew Ondracek, DO2, Joshua Wais, MD3, Joseph Armotrading, MD3, Patrick Stocker, PhD3, Olugbenga Oyesanmi, MD3. P2554 - An Unwanted Neighbor: Contiguous Spread of Colonic Adenocarcinoma, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.