Riddhi Machchhar, DO1, Ibrahim Rahmatullah, MD1, Vera Hapshy, DO2, Hasrshvardhan Sanekommu, MD2, Assif Rozovsky, MD1 1Hackensack Meridian OUMC, Brick, NJ; 2Hackensack Meridian JSUMC, Neptune City, NJ Introduction: A patient with rare breast cancer metastasis to the colon was initially diagnosed with stercoral colitis due to symptoms like abdominal cramping and altered bowel habits. However, further investigation revealed the true cause as breast cancer metastasis. This case underscores the challenges in distinguishing between primary gastrointestinal issues and metastatic disease in breast cancer patients.
Case Description/
Methods: An 84-year-old woman with a history of coronary artery disease, currently on clopidogrel and aspirin, also had stage II invasive ductal carcinoma with extensive lymph node involvement. She underwent right mastectomy and axillary dissection, followed by adjuvant chemotherapy (AC-T) 19 years ago. After poorly tolerating hormonal treatment, she faced a recurrence of cancer in the neck, treated with CyberKnife therapy, radiotherapy, and brief Ixempra chemotherapy until 2012. She was hospitalized for weakness and shortness of breath, she was found to have severe anemia (hemoglobin 6.8) without gross bleeding. An EGD showed congestive gastropathy with no source of anemia. A colonoscopy revealed a 4 mm polyp and a 10 mm ulcer, with the latter biopsied as metastatic breast cancer (ER+/PR-/Her2neu-). A bone marrow biopsy confirmed the diagnosis leading towards a focus on goals of care as surgical intervention is inadvisable. Discussion: Breast cancer is the most prevalent cancer in women in the U.S., comprising 32% of newly diagnosed cancers annually. Metastatic spread primarily targets the bone, lung, and brain, while gastrointestinal (GI) involvement is rare, occurring in only 0.5% of cases. Among GI metastases, the colon and rectum (45%) are most frequently affected, followed by the stomach (28%), small intestine (19%), and esophagus (8%), although some studies claim the stomach as the predominant site (60%).
Symptoms of GI metastasis align with the affected region, with epigastric pain and weight loss common in gastric involvement, and abdominal cramping and occult bleeding in colonic cases. Diagnosis hinges on immunohistochemical markers: breast cancer cells typically express mammaglobin and GATA3, while primary GI malignancies showcase CDX2 and CK20. Given the poor prognosis associated with GI metastasis, treatment strategies focus on palliative care, including hormonal therapy for receptor-positive cases and interventions to alleviate obstruction. Overall survival after diagnosis ranges from 4.7 to 33 months, with a median survival of 33 months observed in a specific cohort.
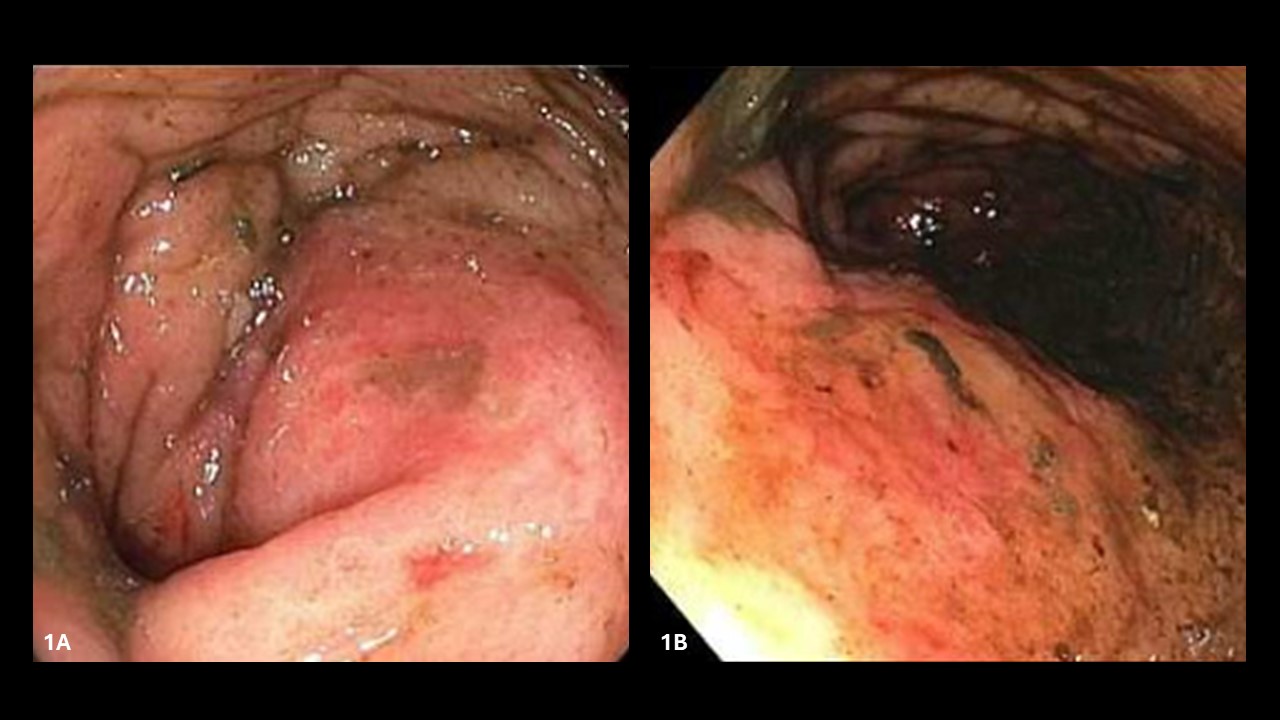
Figure: Figure 1 - Stercoral colitis on colonoscopy
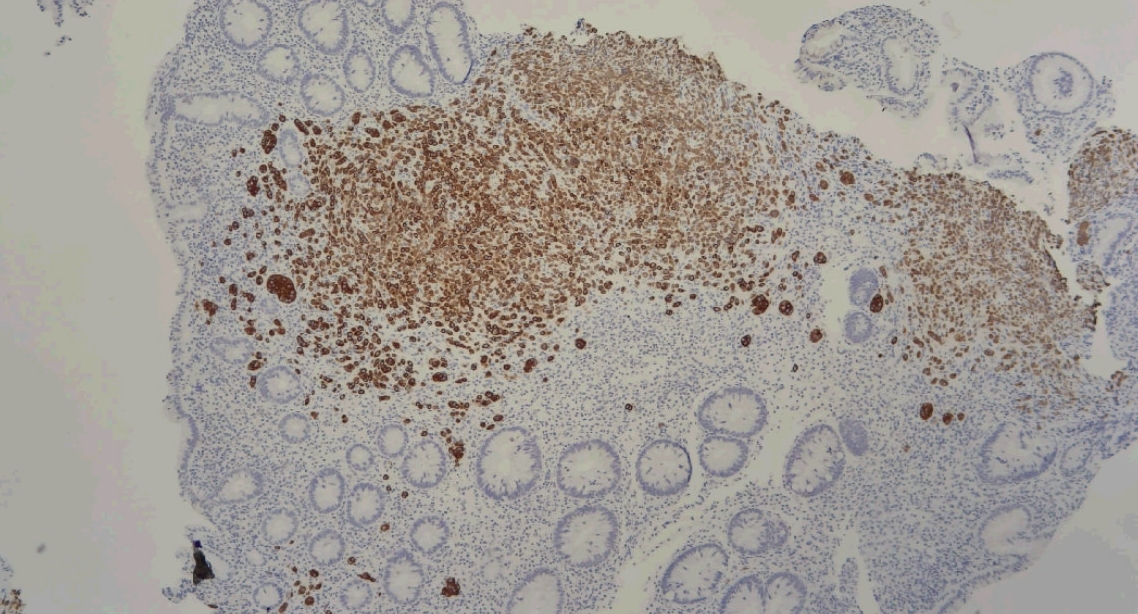
Figure: Figure 2 - Stercoral biopsy results indicating metastatic breast cancer (ER+/PR-/Her2neu-)
Disclosures: Riddhi Machchhar indicated no relevant financial relationships. Ibrahim Rahmatullah indicated no relevant financial relationships. Vera Hapshy indicated no relevant financial relationships. Hasrshvardhan Sanekommu indicated no relevant financial relationships. Assif Rozovsky indicated no relevant financial relationships.
Riddhi Machchhar, DO1, Ibrahim Rahmatullah, MD1, Vera Hapshy, DO2, Hasrshvardhan Sanekommu, MD2, Assif Rozovsky, MD1. P2498 - Unveiling the Unlikely: Stercoral Colitis Masking Rare Breast Metastasis: A Case Report, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")