Department of Internal Medicine, AdventHealth Orlando Orlando, FL
Tareq Alsaleh, MD1, Aimen Farooq, MD2, Dennis Yang, MD, FACG3 1Department of Internal Medicine, AdventHealth Orlando, Orlando, FL; 2Department of Gastroenterology and Hepatology, AdventHealth Orlando, Orlando, FL; 3Center for Interventional Endoscopic, AdventHealth Orlando, Orlando, FL Introduction: Pancreatic ductal adenocarcinoma (PDAC) is the most common pancreatic malignancy. Anaplastic T-cell lymphoma (ALCL) is another, much rarer tumor that has different management and prognosis. Here, we present a rare case of ALCL of the pancreatic head.
Case Description/
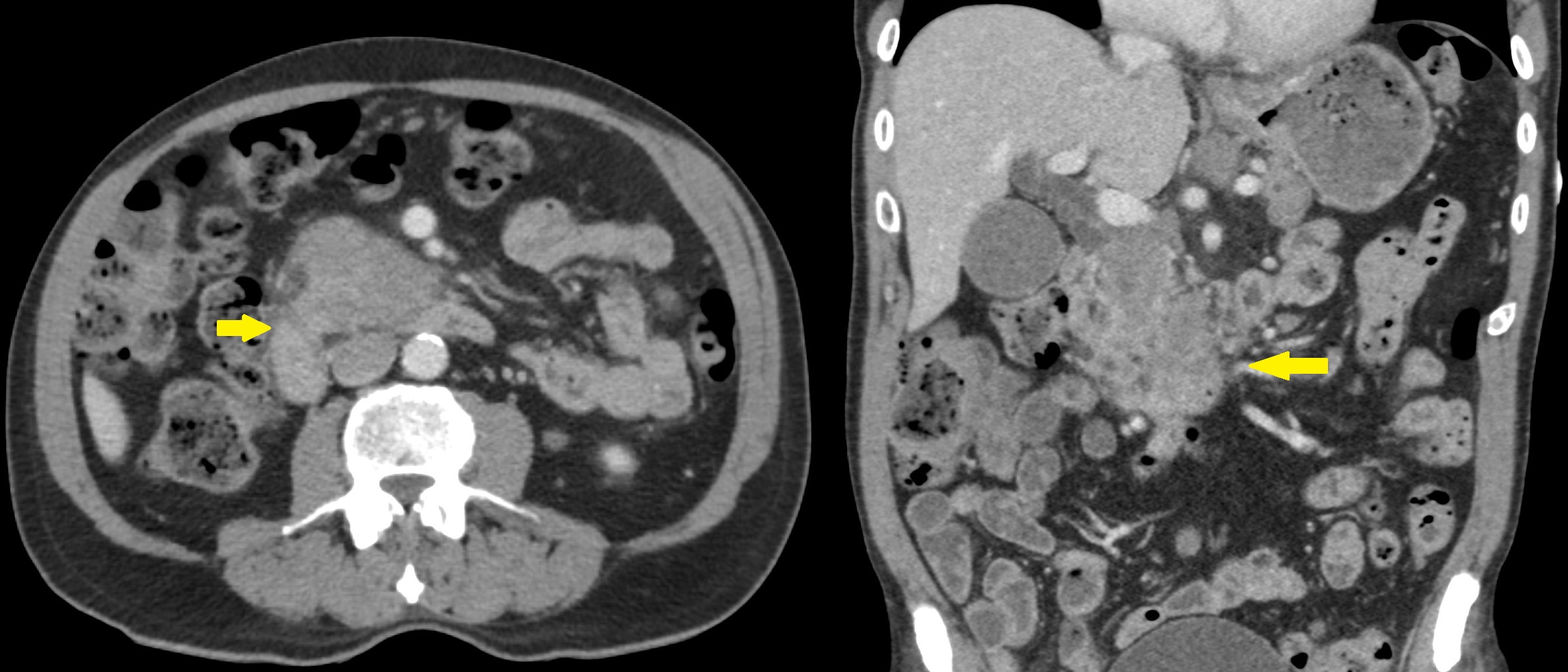
Methods: An 81-year-old male presented to the emergency department with a three-week history of dull epigastric pain and nausea. Physical examination revealed normal vital signs, abdominal tenderness, and multiple palpable subcutaneous nodules with overlying erythema on the left chest and back. Laboratory tests showed a lipase of 700 U/L, ALT of 138 U/L, AST of 157 U/L, bilirubin of 2.2 mg/dL, and ALP of 206 U/L. Carbohydrate antigen 19-9 level was high at 84.8 U/mL. Computed tomography showed widespread lymphadenopathy and a 5 x 4 cm mass of the head/uncinate process resulting in upstream biliary ductal dilation (Figure 1).
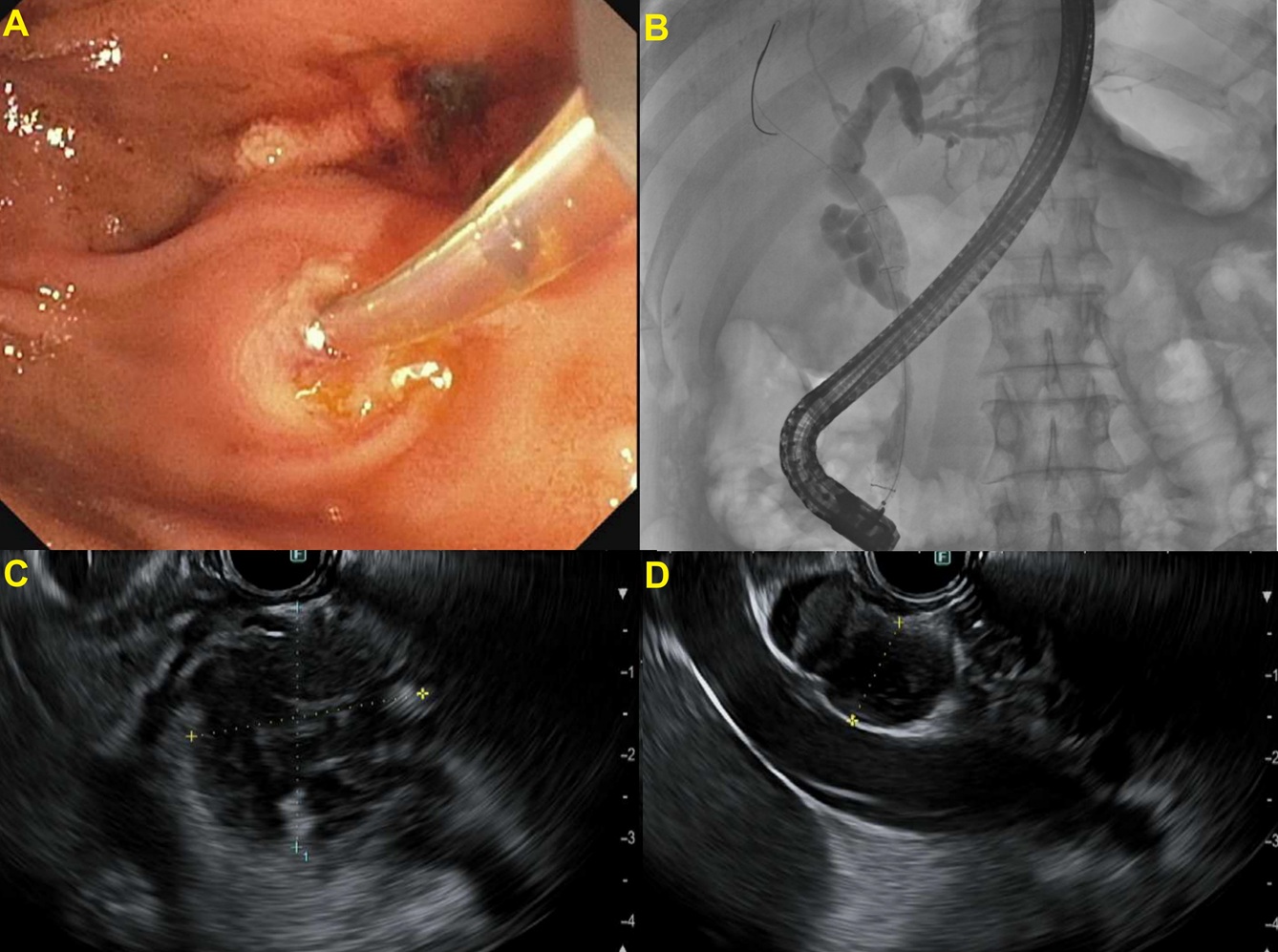
Endoscopic retrograde cholangiopancreatography showed a main bile duct malignant stricture with upstream dilation. A biliary sphincterotomy was performed with subsequent placement of a covered metal stent. The ampulla appeared normal without surrounding masses. Endoscopic ultrasound showed a heterogenous, hypoechoic pancreatic head mass with irregular borders (Figure 2). Fine-needle aspiration (FNA) revealed ALCL staining positive for CD30 and negative for anaplastic lymphoma kinase (ALK).
He was offered chemotherapy, but he opted for hospice care at home. Discussion: Pancreatic lymphoma (PL) can be primary (PPL), originating in the pancreas, or secondary (SPL), due to metastasis from a distant source. The distinction between the two is based on clinical and radiologic criteria, as their pathological features are identical.
A pancreatic mass with peripancreatic lymphadenopathy, in the absence of superficial or mediastinal lymph node involvement, hepatic lesions, or splenic infiltration, is highly suggestive of PPL. The wide subcutaneous, multi-organ, and lymphatic spread in our case favors SPL, which is most commonly from a nodal source. Notably, the large size of his pancreatic mass is not typical of secondary dissemination. The patient chose hospice care, limiting further evaluation to unravel the primary source.
Unlike the management of PDAC, which relies on curative resection, ALCL is treated with chemotherapy and carries a better prognosis. The identification of ALK helps stratify ALCL into ALK-positive and ALK-negative tumors. The former has a favorable prognosis due to the potential for targeted therapy.
Figure: Figure 1. A confluent mass-like appearance of the head/uncinate process, with many small omental, mesenteric, retroperitoneal, and perinephric nodules, indicating metastatic disease.
Figure: Figure 2. A – Major papilla appeared normal. B - A single segmental biliary stricture was found in the lower third of the main bile duct. The stricture was malignant appearing. The entire biliary tree was moderately dilated. C – An irregular hypoechoic mass measuring 37 by 27 mm identified in the pancreatic head. D – Abnormal hypoechoic lymph nodes visualized in the peri-pancreatic region and perigastric region
Disclosures: Tareq Alsaleh indicated no relevant financial relationships. Aimen Farooq indicated no relevant financial relationships. Dennis Yang: 3D-Matrix – Consultant. Apollo Endosurgery – Consultant. ERBE – Consultant. Fujifilm – Consultant. Medtronic – Consultant. MicroTech – Consultant. Olympus – Consultant.
Tareq Alsaleh, MD1, Aimen Farooq, MD2, Dennis Yang, MD, FACG3. P2361 - Chicken or Egg? The Paradox of a Large Pancreatic Lymphoma with Systemic Spread, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.