Fady Gendy, DO, Neria Bitton, MD, Alex Caplan, DO, Deepa Kumarjiguda, DO, David L.. Diehl, MD, Alana Persaud, MD Geisinger Health System, Danville, PA Introduction: Solid pseudopapillary neoplasm (SPN) of the pancreas is a rare benign tumor constituting up to 2.7% of all pancreatic neoplasms and occurring predominantly in young females. Mostly occurring in the tail or body of the pancreas and presenting asymptomatically, these tumors can degenerate over time causing intratumor bleeding and cyst formation but also have metastatic potential. Additionally, there have been less than 10 reported cases of SPN presenting as acute pancreatitis as we present here. Surgical intervention is generally favorable, however metastatic transformation carries a poor prognosis. We highlight SPN presenting as acute pancreatitis in a 27-year-old female one month post cesarean delivery.
Case Description/
Methods: A 27-year-old, female presented with sharp epigastric pain one month after scheduled cesarean delivery. Labs revealed an elevated lipase of 221 U/L, concerning for acute pancreatitis. A CT of the abdomen and pelvis identified a 9.5 cm mixed cystic and solid mass in the pancreas inseparable from the stomach with an enhancing component. Also noted were mesenteric and retroperitoneal inflammation suggestive of acute pancreatitis. Endoscopic ultrasound with fine needle biopsy (FNB) returned positive for CTNNB1 mutation, CD10, synaptophysin, and beta-catenin, confirming SPN. The patient underwent successful distal pancreatectomy and splenectomy 3 weeks after the diagnosis. Discussion: Though literature is limited, review shows that SPN mean tumor size is 45 mm with tumors greater than 50 mm in diameter being associated with possibly an increased malignant or aggressive behavior. We highlight a case of SPN presenting as acute pancreatitis, measuring at 100 x95 x 85 mm suggesting a more aggressive neoplasm. The large tumor size as in our case, may have caused acute pancreatitis due to rapid enlargement from intratumor hemorrhage leading to ischemia and obstruction of the pancreatic duct, as this was also noted in similar cases with larger tumors. To further support this, our pathology results confirmed cystic areas with bloody fluid. It is unclear if pregnancy had a role in our patient’s presentation, though it is possible symptoms could have been masked by pregnancy and delayed the diagnosis. SPNs are associated with an excellent prognosis, with high survival rates exceeding 95% after complete surgical removal. Long-term outcomes remain favorable even in cases of advanced or metastatic disease.
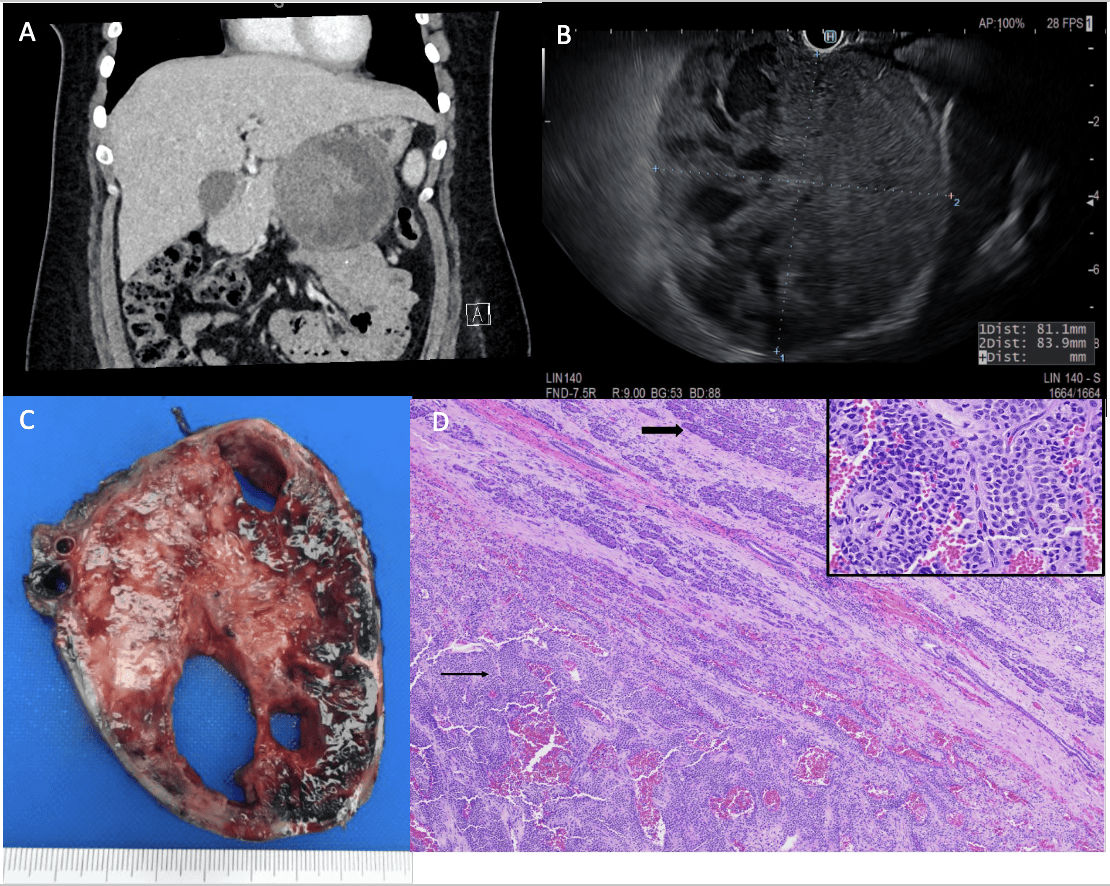
Figure: A. CT imaging shows large heterogenous cystic structure adjacent to stomach and pancreas. B. Endoscopic ultrasound images confirm cystic and solid components. C. Distal pancreatectomy specimen grossly shows a 10.0 x 9.5 x 8.5 cm large, encapsulated mass with focally cystic and focally solid areas. The cystic areas are filled with a bloody fluid and the solid areas are tan-pink, congested, hemorrhagic and focally necrotic. Tumor involves most of the pancreas. D. Distal subtotal pancreatectomy specimen shows a rim of normal pancreatic parenchyma (large arrows) and the well-circumscribed mass composed of solid monomorphic sheets of polygonal cells admixed within delicate vessels surrounded by hyalinized stroma and degenerative changes (thin arrow) (Hematoxylin and Eosin (H&E), 4x objective, 40x magnification). Inset shows solid pseudopapillary neoplasm (SPN) cells with salt and pepper neuroendocrine type chromatin on high power magnification (H&E, 400x).
Disclosures: Fady Gendy indicated no relevant financial relationships. Neria Bitton indicated no relevant financial relationships. Alex Caplan indicated no relevant financial relationships. Deepa Kumarjiguda indicated no relevant financial relationships. David Diehl indicated no relevant financial relationships. Alana Persaud indicated no relevant financial relationships.
Fady Gendy, DO, Neria Bitton, MD, Alex Caplan, DO, Deepa Kumarjiguda, DO, David L.. Diehl, MD, Alana Persaud, MD. P2344 - The Largest Known Case of a Solid Pseudopapillary Neoplasm Presenting as Acute Pancreatitis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.