University of Minnesota Medical Center Minneapolis, MN
Peter Kim, MD1, Ying Gibbens, MD, PhD1, Daniela Guerrero Vinsard, MD2 1University of Minnesota Medical Center, Minneapolis, MN; 2University of Minnesota and Minneapolis VA Health Care System, Minneapolis, MN Introduction: Autoimmune pancreatitis (AIP) diagnosis is challenging as it mimics pancreaticobiliary malignancies. When patients present with AIP features but fail to satisfy HISORt criteria (histology, imaging, serology, other organ involvement, response to steroids), alternative etiologies including distant malignancies should be considered. We present renal mucosa-associated lymphoid tissue (MALT) lymphoma closely mimicking AIP when classic criteria are not met.
Case Description/
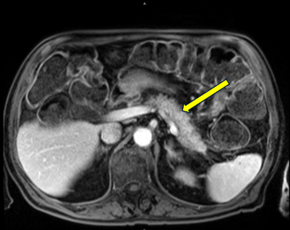
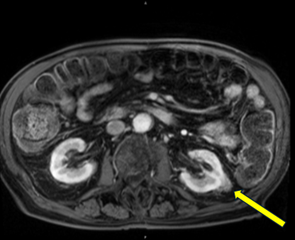
Methods: An 87-year-old man presented with steatorrhea and 15-pound weight loss for 3 months. Initial workup including thyroid studies, lipase, celiac serology were normal. Fecal elastase was low (< 15 μg/g; normal >200 μg/g). Colonoscopy ruled out inflammatory bowel disease and microscopic colitis. The patient had no pancreatic insufficiency risk factors. Pancreatic enzyme replacement provided modest improvement but weight loss persisted. Three months later, he was hospitalized for hyperosmolar hyperglycemic state (HbA1c 10.2%) with new type 2 diabetes. MRI showed diffuse pancreatic inflammation with feathery appearance without masses. IgG4 was mildly elevated at 154 mg/dL (normal 6-121 mg/dL). Endoscopic ultrasound revealed pancreatic lobularity with lesions, but fine needle biopsy failed to yield pancreatic cells. Follow-up MRI showed persistent pancreatic inflammation and incidental renal mass. Biopsy revealed MALT lymphoma. PET-CT demonstrated uptake in both renal mass and pancreatic tissue, suggesting infiltration. Rituximab was initiated with repeat PET-CT showing decreased uptake in both locations.
Discussion: This highlights the diagnostic challenge when clinical presentations suggest AIP but HISORt criteria are not met. While the patient had pancreatic inflammation, modest IgG4 elevation, and insufficiency, absence of classical enlargement, significantly elevated IgG4 ( > 2 times upper limit), or histologic confirmation left AIP diagnosis equivocal. Renal MALT lymphoma provided an alternative explanation. PET-CT uptake in both renal mass and pancreatic tissue strongly suggests lymphomatous pancreatic infiltration, potentially explaining combined endocrine and exocrine insufficiency. This is supported by transient endocrine dysfunction resolving spontaneously, exocrine improvement, and concordant treatment response. No documented cases exist of renal MALT lymphoma affecting pancreas, making this case unique. This underscores maintaining broad differential diagnoses when evaluating suspected AIP with unmet HISORt criteria.
Figure: Inflammation of the Pancreatic Body
Figure: Enhancing Soft Tissue Mass of Left Kidney
Disclosures: Peter Kim indicated no relevant financial relationships. Ying Gibbens indicated no relevant financial relationships. Daniela Guerrero Vinsard indicated no relevant financial relationships.
Peter Kim, MD1, Ying Gibbens, MD, PhD1, Daniela Guerrero Vinsard, MD2. P2306 - When the Kidney Speaks for the Pancreas: MALT Lymphoma Masquerading as Autoimmune Pancreatitis, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.