St. Luke's University Health Network Bethlehem, PA
Bryan Wey, MD, Ronak Modi, MD St. Luke's University Health Network, Bethlehem, PA Introduction: Pancreatic neuroendocrine tumors (pNETs) are rare causes of pancreatic tumors. Functional tumors can be categorized into hormones that they secrete, such as insulinomas, gastrinomas, glucagonomas, etc. Non-functional tumors are typically discovered incidentally on imaging due to their indolent nature; they are not associated with clinical syndrome of hormone hypersecretion. Symptoms, if present, are due to mass effect from advanced tumor stage with metastatic spread. Here we discuss a case of a patient who developed Zollinger-Ellison syndrome from recurrent pNET after initial resection.
Case Description/
Methods: An 88-year-old male underwent abdominal imaging for further evaluation of a hepatic cyst, which showed a 4 cm enhancing mass in the pancreatic tail. He underwent endoscopic ultrasound (EUS) and fine needle aspiration demonstrated well-differentiated pNET. Follow-up DOTATATE-enhanced PET scan showed intense radiotracer uptake in the pancreatic tail and a peripancreatic lymph node. He underwent distal pancreatectomy and lymph node dissection; pathology showed G2 pNET with negative margins and 6/8 regional lymph nodes involved. After the surgery he developed progressively worsening diarrhea that somewhat improved with pancreatic enzyme replacement therapy. He did not tolerate octreotide injections, as it worsened his diarrhea. Chromogranin A was elevated 6 months after surgery and continued to rise on subsequent monitoring. Repeat imaging showed a nodule at the resection site and a retroperitoneal lymph node with radiotracer avidity consistent with recurrence. He presented to the hospital for worsening of his chronic diarrhea and melena. EGD was performed and showed multiple clean-based duodenal ulcers, some of which were distal to the ampulla, raising concern for Zollinger-Ellison syndrome. Gastrin level was 2851. He started on lanreotide with subsequent improvement in his diarrhea and tumor markers. Discussion: Transformation of a non-functional pNET into a hormone-producing tumor is rarely described in the literature. Although the underlying mechanism of functional transformation is poorly understood, it is an important phenomenon for clinicians to be aware of. Local disease is typically managed via surgical resection. Medical management for gastrinomas include high dose acid suppression and somatostatin analogs to reduce hormone production. Advanced/metastatic disease may require the systemic treatments such as chemotherapy, molecular therapy or peptide receptor radioligand therapy.
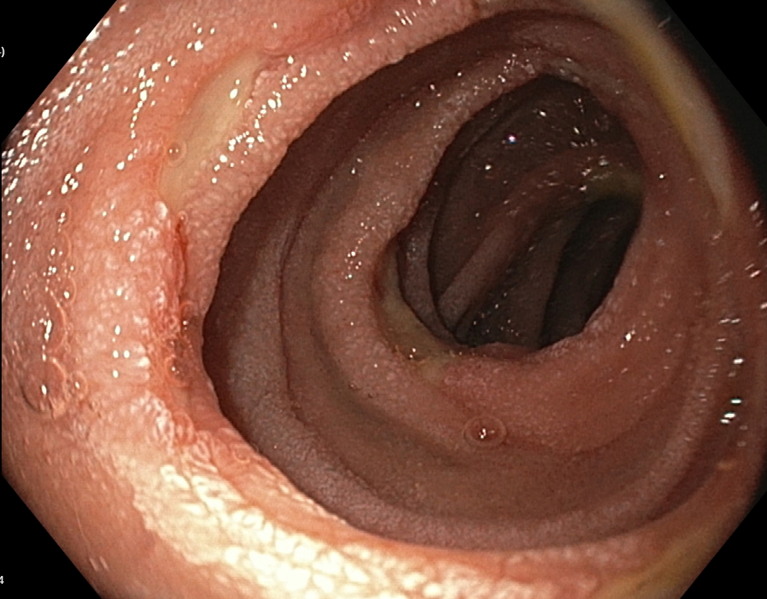
Figure: Figure 1. Multiple clean-based ulcers seen in the distal duodenum
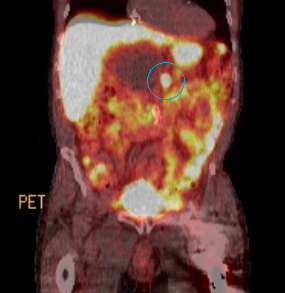
Figure: Figure 2: Post-surgical DOTATATE PET scan showing recurrent pNET at the prior pancreatic resection site
Disclosures: Bryan Wey indicated no relevant financial relationships. Ronak Modi indicated no relevant financial relationships.
Bryan Wey, MD, Ronak Modi, MD. P2270 - Recurrent Pancreatic Neuroendocrine Tumor With Functional Transformation, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.