Infirmary Health - Mobile Infirmary Medical Center Mobile, AL
Brandon E. Newell, DO1, Bennett S. Hooks, MD2 1Infirmary Health - Mobile Infirmary Medical Center, Mobile, AL; 2Infirmary Health, Mobile, AL Introduction: A pancreatico-pleural fistula (PPF) is a rare complication of pancreatitis that arises from disruption of the pancreatic ductal system or from extension of a pancreatic pseudocyst into the pleural space. We present the case of a patient with a PPF in the setting of alcohol induced chronic pancreatitis and complete pancreatic divisum (PD), with endoscopic management that has not previously been reported to our knowledge.
Case Description/
Methods: A 34 year old male with a history of alcohol induced chronic pancreatitis presented to the ED following an episode of binge drinking with 4 days of shortness of breath, abdominal pain, nausea and vomiting. A CTA chest and CT abdomen were obtained which revealed a large left pleural effusion with near complete atelectasis of the left lung and findings consistent with chronic pancreatitis, massive dilation of the main pancreatic duct and a likely fistulous tract from the pancreatic duct to the mediastinum. Left thoracentesis was performed, the pleural effusion was persistent and a 24 Fr chest tube was placed. Pleural fluid analysis revealed an elevated amylase > 1,000, consistent with a PPF. The patient underwent ERCP which revealed complete PD, the dorsal pancreatic duct had an initial area of stricture followed by massive ductal dilation. Serial dilation was performed and a pancreatic duct plastic stent was placed. In a staged fashion, the patient underwent a repeat ERCP 7 days later, with further serial dilation and replacement of the stent with a self-expanding covered metal stent. Due to the expansive nature of the pleural effusion the patient also underwent a left video assisted thoracoscopy with evacuation and decortication. At follow up, 2 weeks after discharge the patient was doing well without evidence of reaccumulating pleural effusion. Plan is for the patient to follow up at a 3 month interval for ERCP and stent removal. Discussion: We present management of a rare presentation of PPF in the setting of complete PD, managed with a staged procedure including sphincterotomy, pancreatic duct plastic stent placement, further serial dilation and placement of a covered metal stent through the minor papilla to restore natural pancreatic flow and divert pancreatic secretions from the fistulous tract. Of the similar cases described in the literature ours is the only that describes treatment of a dorsal pancreatic stricture through the minor papilla.
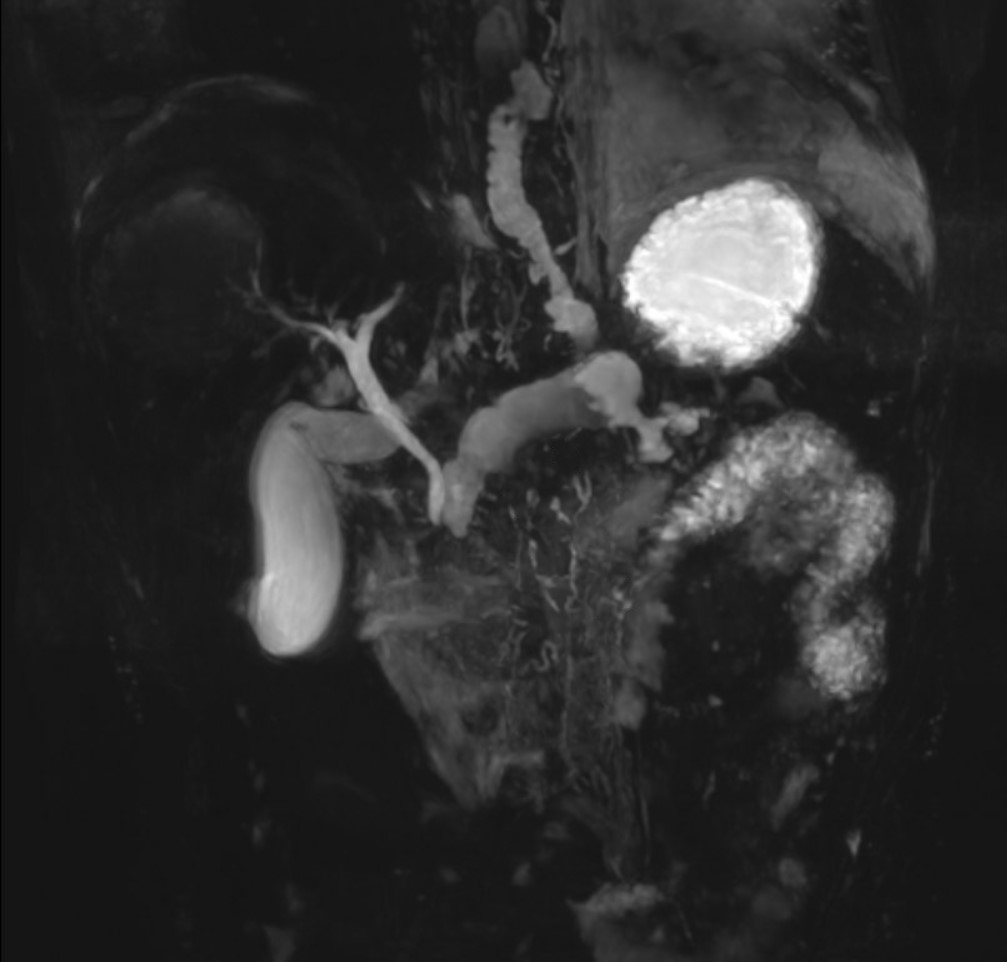
Figure: Figure 1. MRCP showing evidence of possible complete pancreatic divisum and a dilated pancreatic duct with fistulous communication into the mediastinum.
Figure: Figure 2. ERCP via cannulation of the minor papilla, showing massive dilation of the dorsal pancreatic duct and evidence of complete pancreatic divisum.
Disclosures: Brandon Newell indicated no relevant financial relationships. Bennett Hooks indicated no relevant financial relationships.
Brandon E. Newell, DO1, Bennett S. Hooks, MD2. P2263 - A Major Problem Treated Through the Minor Papilla: Endoscopic Management of a Pancreatico-Pleural Fistula via the Minor Papilla, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")