Inoushka Mejias-Rovira, MD, Alondra Velez-Santiago, MD, Juan G. Feliciano-Figueroa, MD, Kyara M. Ostolaza-Oquendo, MD, Jose Martin-Ortiz, MD, FACG VA Caribbean Healthcare System, San Juan, Puerto Rico Introduction: Diffuse large B-cell lymphoma (DLBCL) is the most common form of non-Hodgkin lymphoma, accounting for 30% of all lymphoma cases. Extranodal involvement occurs in up to 40% of cases, with the gastrointestinal tract being the most frequent site. Gastric DLBCL can mimic other malignancies, including pancreatic adenocarcinoma, complicating diagnosis. Timely identification through endoscopy and biopsy is essential, as treatment delays can worsen outcomes. We present a case of a non-germinal center DLBCL initially suspected to be pancreatic cancer until a diagnostic biopsy unmasked the true nature of the malignancy.
Case Description/
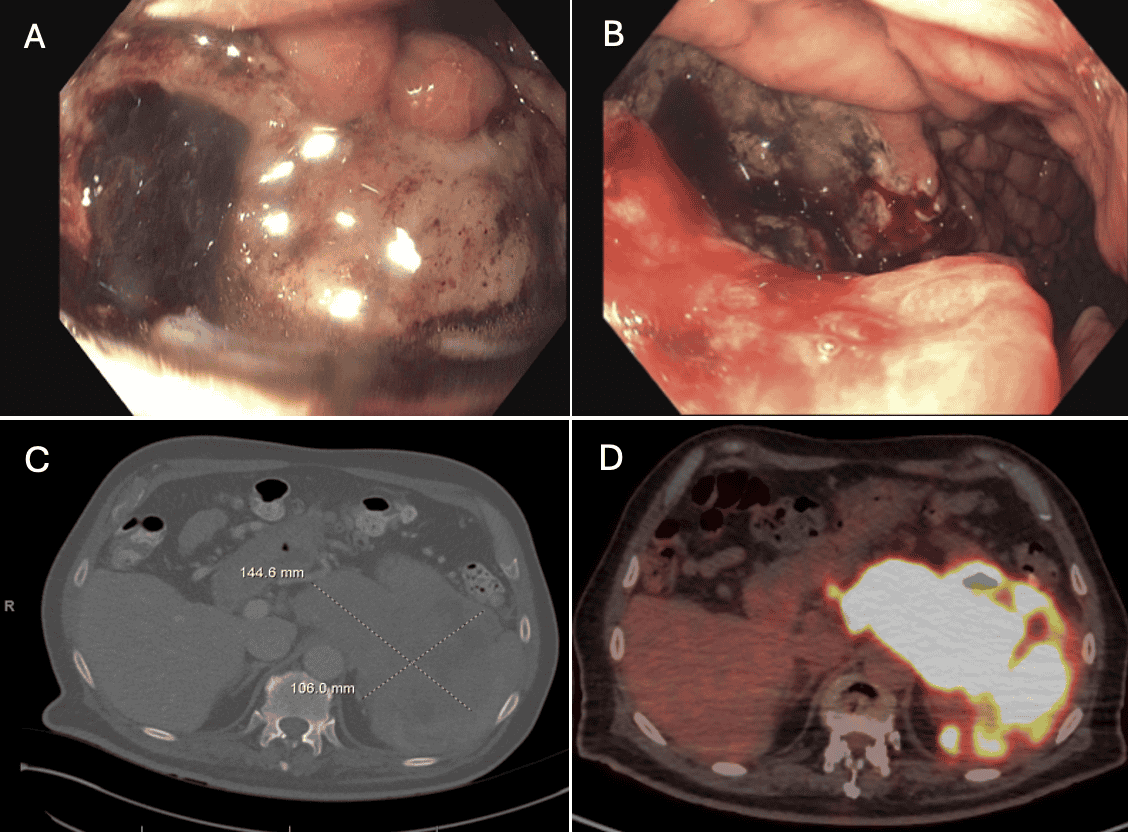
Methods: A 77-year-old man presented with an 8-month history of vague abdominal pain, early satiety, unintentional weight loss, fatigue, and 3 months of melena. His medical history was unremarkable. Family history was notable for a first-degree relative with pancreatic cancer. An outpatient MRI showed a large intra-abdominal mass arising either from the pancreatic body or the posterior wall of the stomach, prompting referral for further evaluation. Upper endoscopy revealed a large ulcerated, necrotic mass involving the gastric cardia, fundus and greater curvature (Figure 1A-B). Biopsies were taken and staging imaging was performed. CT scan of the chest, abdomen and pelvis demonstrated a substantial gastric mass in the left upper quadrant, extending into and encasing the pancreas and spleen, along with pulmonary nodules, a splenic lesion and retroperitoneal lymphadenopathy (Figure 1C). These findings strongly suggested metastatic pancreatic adenocarcinoma. However, histopathological analysis of the gastric biopsy identified non-germinal center DLBCL, fundamentally altering the diagnosis and management. Discussion: This case is remarkable for the extent of gastric involvement and its mimicry of pancreatic cancer. The size of the mass and invasion of adjacent organs initially pointed to a poor prognosis carcinoma. Yet, biopsy confirmed a treatable lymphoma, highlighting the critical role of tissue diagnosis in cases with overlapping clinical and imaging features. This highlights how histopathology can dramatically redirect clinical management, particularly in malignancies like DLBCL where prompt initiation of chemotherapy significantly improves outcomes.
Figure: Figure: 1A-B: Large ulcerated mass in gastric body and fundus with stigmata of recent bleeding, respectively. 1C: Abdominopelvic CT with IV contrast showing a large ill-defined heterogeneously enhancing mass at the left upper quadrant, measuring 14.5x10.5cm. 1D: Hypermetabolic lesions in the left upper quadrant with involvement of the spleen, stomach and pancreas.
Disclosures: Inoushka Mejias-Rovira indicated no relevant financial relationships. Alondra Velez-Santiago indicated no relevant financial relationships. Juan Feliciano-Figueroa indicated no relevant financial relationships. Kyara Ostolaza-Oquendo indicated no relevant financial relationships. Jose Martin-Ortiz indicated no relevant financial relationships.
Inoushka Mejias-Rovira, MD, Alondra Velez-Santiago, MD, Juan G. Feliciano-Figueroa, MD, Kyara M. Ostolaza-Oquendo, MD, Jose Martin-Ortiz, MD, FACG. P2116 - Ulcerated Gastric Mass Masquerading as Pancreatic Cancer: A Case of Non-Germinal Center Diffuse Large B-cell Lymphoma, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.