Alondra Velez-Santiago, MD, Orlando Rodriguez-Amador, MD, Loscar Santiago-Rivera, MD VA Caribbean Healthcare System, San Juan, Puerto Rico Introduction: Gastroparesis is a chronic gastrointestinal motility disorder characterized by delayed gastric emptying in the absence of mechanical obstruction. While most cases are attributed to diabetes, post-surgical changes, or idiopathic, infectious causes are rare and overlooked. Sarcina ventriculi is a gram-positive anaerobic bacterium that has been sporadically reported in association with gastric disorders. This case highlights an unusual instance of gastroparesis where S. ventriculi was identified on histological examination.
Case Description/
Methods: A 45-year-old male presented to the gastroenterology clinic with intermittent dyspepsia, constipation, and abdominal pain. He was clinically stable, with a benign abdominal examination, had longstanding gastroesophageal reflux symptoms ( >20 years), and no prior history of endoscopy or H. pylori testing. The patient had no history of diabetes mellitus or use of GLP-1 receptor agonists.
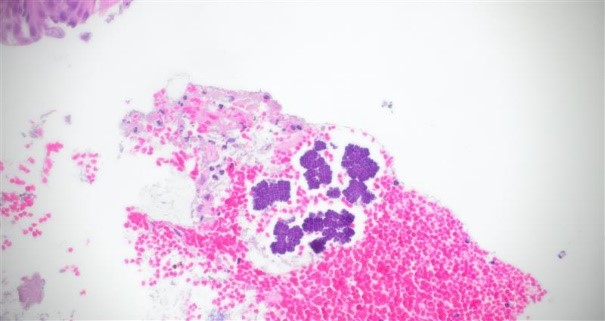
Upper endoscopy revealed two polypoid lesions in the gastric cardia (biopsied) and a large amount of food residue in the stomach, despite the patient reporting he had been NPO since 6:00 p.m. the previous evening. Biopsies showed admixed vegetable material and structures most consistent with Sarcina ventriculi. Infectious disease consultation was obtained given the limited literature on this organism. Based on clinical presentation, the patient was treated with oral metronidazole 500 mg for 10 days.
At the three-month follow-up, the patient reported complete resolution of symptoms. Repeat upper endoscopy with biopsy showed no recurrence of the organism and decreased gastric inflammation. Discussion: The detection of S. ventriculi should prompt clinicians to consider infectious contributions, more in patients with unexplained gastroparesis symptoms and no risk factors for delayed gastric emptying. While the clinical significance of Sarcina remains debated, its association with serious complications such as emphysematous gastritis and perforation highlights the importance of early identification and management.
Currently, no standardized treatment protocol exists for S. ventriculi eradication. Reported antibiotic regimens include metronidazole, ciprofloxacin, amoxicillin-clavulanate, penicillin, or tetracyclines, often combined with proton pump inhibitors to reduce gastric acidity. Further studies are needed to clarify the pathogenic mechanisms and to establish when antimicrobial treatment is warranted. Until then its presence in gastroparesis cases should not be dismissed.

 photo")