University of Pittsbugrh Medical Center Flushing, NY
Christina Tache, MD1, Hareem Fatima, MD2, Hafsah Ali, MBBS3, Muhammad Usama Bin Shabbir, MBBS4 1University of Pittsbugrh Medical Center, Flushing, NY; 2: Federal Government Polyclinic, Islamabad, Pakistan, Islamabad, Islamabad, Pakistan; 3Allama Iqbal Medical College, Manama, Al Muharraq, Bahrain; 4Pakistan Institute of Medical Sciences, Shaheed Zulfiqar Ali Bhutto Medical University, Multan, Punjab, Pakistan Introduction: Splenic abscesses are very rare and can lead to severe complications if not treated promptly. We report a case of an isolated splenic abscess in an otherwise healthy 18-year-old male, with blood cultures identifying Shigella flexneri (S. flexneri). The patient was treated conservatively with intravenous (IV) antibiotics and his symptoms resolved. Although splenectomy previously was regarded as the "gold standard" treatment, the trend is now moving towards a more conservative approach.
Case Description/
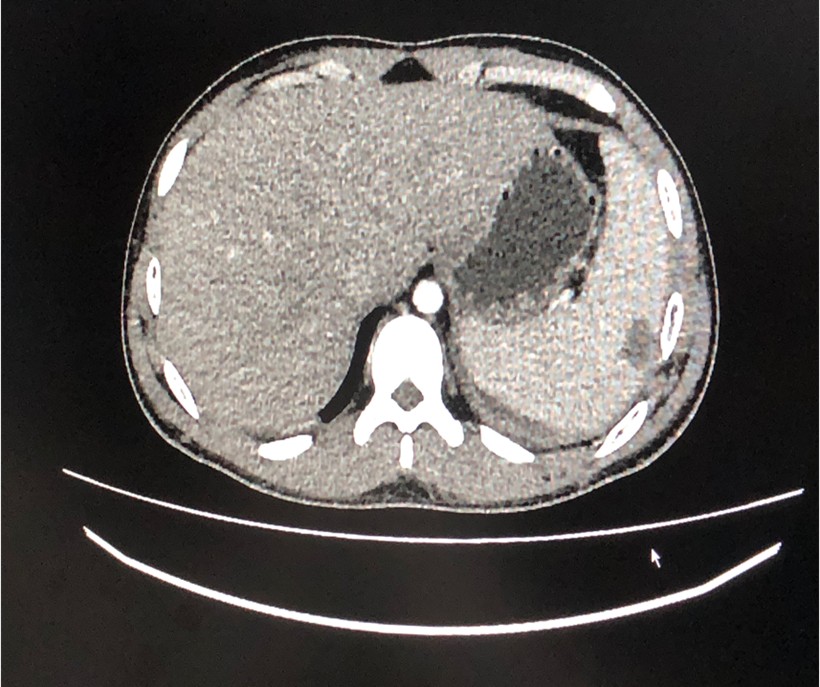
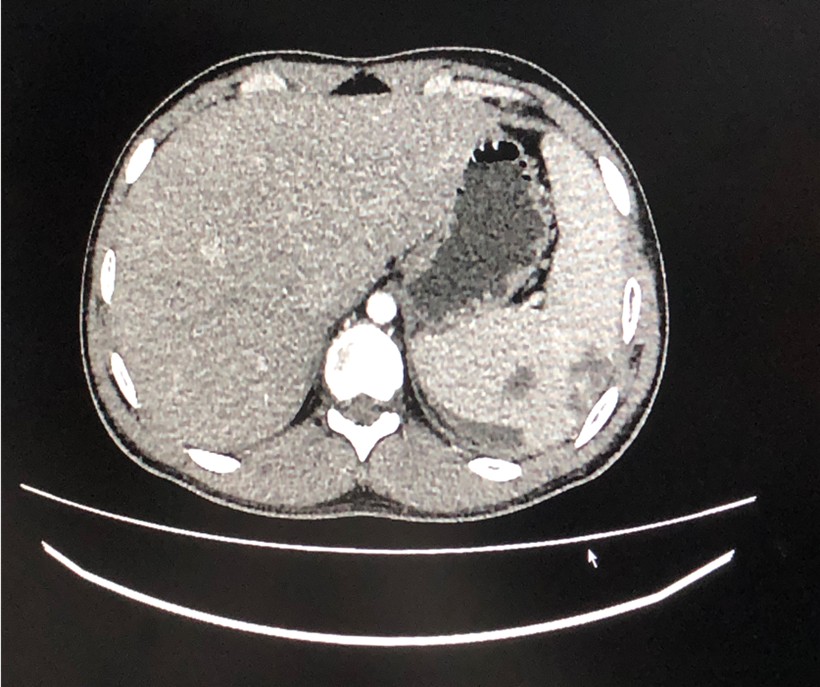
Methods: An 18-year-old male, working as a farmer, presented to the emergency department with a 2-week history of low-grade fevers, 3 days dull upper abdominal pain, and 2 days vomiting/diarrhea. The patient had been taking over-the-counter antipyretics and ciprofloxacin and cefixime for 4 days at home with no improvement. There was no history of trauma, recent blood transfusion, exposure to cattle and poultry, or unpasteurized milk consumption. There was a notable family history of a paternal cousin who was treated for a splenic abscess. On admission, vitals signs revealed he was febrile (100.4°F), heart rate 105, and blood pressure 90/60 mmHg. Abdominal exam showed a soft, non-distended abdomen with mild tenderness in the epigastric region and left upper quadrant. Pertinent labs included WBC 13.6 x 109/L, neutrophils 87.8%, CRP 92 mg/L, Hb 14 g/L, ALT 262 U/L, and AST 211 U/L. Abdominal US showed hepatosplenomegaly with spleen measuring 13 cm with multiple peripheral hypoechoic wedge-shaped areas measuring 46x25 mm and intraparenchymal lesions measuring 21x12 mm. Abdominal CT imaging showed hypodense linear splenic areas, likely splenic abscess. He was empirically treated for enteric fever with ceftriaxone and azithromycin while awaiting blood culture results. Despite treatment, he remained febrile and experienced worsening abdominal pain. When patient did not show improvement, meropenem was added. Blood cultures identified S. flexneri. The patient was switched to IV sulzone and vancomycin and responded well and was afebrile by the sixth day of admission. The patient continued IV antibiotics for 4 weeks and was discharged with a 14-day course of oral linezolid and moxifloxacin, with an outpatient follow-up appointment. Discussion: Splenic abscesses are extremely uncommon; autopsy studies revealed their prevalence to be between 0.2%-0.7%. There is no universally accepted standard for managing splenic abscesses; instead, treatment should be tailored to the specific needs of each individual patient.
Figure: CT abdomen showing splenic lesion
Figure: CT abdomen showing splenic lesion
Disclosures: Christina Tache indicated no relevant financial relationships. Hareem Fatima indicated no relevant financial relationships. Hafsah Ali indicated no relevant financial relationships. Muhammad Usama Bin Shabbir indicated no relevant financial relationships.
Christina Tache, MD1, Hareem Fatima, MD2, Hafsah Ali, MBBS3, Muhammad Usama Bin Shabbir, MBBS4. P2108 - Isolated Splenic Abscess Due to Shigella Flexneri in a Healthy Young Man: A Case Report, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

.jpg "Christina Tache, MD photo")