Khandokar A. Talib, MD1, Ahmed Shehadah, MD2, Usama Sakhawat, MD3, Khadija Raza, MD3, Godson Senyendo, MD4, Rahat Elahi, 5, Minhaz Ahmad, MD1, Ali Marhaba, MD4 1United Health Services, Wilson Medical Center, Vestal, NY; 2United Health Services, Wilson Medical Center, Binghamton, NY; 3United Health Services Hospital, Johnson City, NY; 4United Health Services, Wilson Medical Center, Johnson City, NY; 5SUNY Downstate Health Sciences University, East Elmhurst, NY Introduction: Gastric pneumatosis (GP) is a rare condition typically precipitated by forceful retching, gastric trauma, gastric outlet obstruction, gastric ulcers, and mucosal necrosis, leading to air trapping within the stomach wall. GP should be distinguished from emphysematous gastritis, which can have different precipitant causes, including hematogenous spread or direct inoculation. GP can lead to hepatic portal venous gas. Hereby, we present a case of GP and highlight its diagnosis, endoscopic findings, and management, which may help guide future cases.
Case Description/
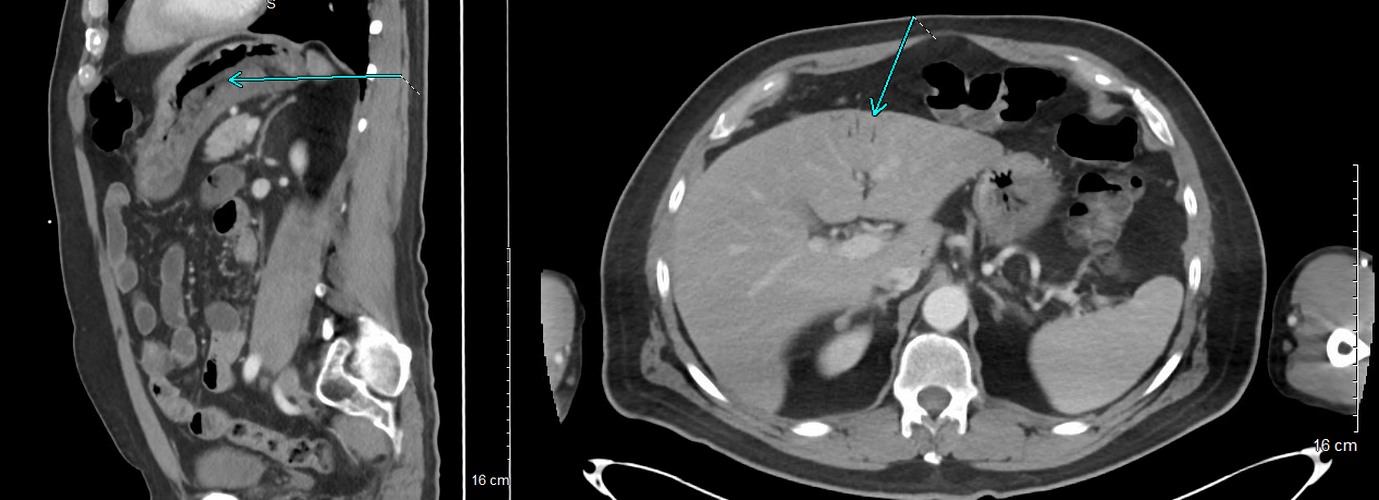
Methods: A 70-year-old male with a past medical history of essential hypertension, gastroesophageal reflux disease, and diverticulosis presented to the emergency department with a two-day history of sudden-onset epigastric abdominal pain, nausea, and vomiting. He denied similar symptoms in the past, chronic use of over-the-counter pain medications, fever, or diarrhea. Vital signs were within normal limits. Abdominal examination revealed mild epigastric tenderness but was otherwise unremarkable. Laboratory results were notable for mild hyponatremia, hypokalemia, elevated bicarbonate, and mildly elevated liver enzymes, with normal alkaline phosphatase and total bilirubin. Amylase, lipase, and lactic acid levels were within normal limits. CT abdomen and pelvis demonstrated gastric pneumatosis along the greater curvature starting from the fundus, along with Hepatic Portal Venous Gas (HPVG) extending into the left hepatic lobe (Figure 1). Mesenteric vessels were widely patent, with no evidence of free intraperitoneal air. Scattered diverticulosis was also noted. The patient was managed conservatively with NPO, IV fluids, PPI, and an antiemetic. Upper endoscopy revealed a normal esophagus, a small hiatal hernia, and diffuse severe inflammation with congestion and erythema involving the gastric fundus, body, and antrum (Figure 2). Erythematous duodenopathy was also noted. Biopsies from the stomach revealed chronic inactive gastritis, negative for H. pylori. Surgical consultation endorsed continued conservative management. The patient experienced symptomatic improvement and was subsequently discharged. Discussion: The above patient, with clinical presentation and CT findings of GP and HPVG, likely developed these due to forceful retching from a viral illness and improved with conservative care. Surgical intervention should be reserved for patients with clinical deterioration or complications such as perforation or necrosis.
Figure: Figure 1: Gastric pneumatosis along the greater beginning at the fundus, portal venous gas extended in the liver.
Figure: Figure 2: Diffuse severe inflammation characterized by congestion and erythema in the gastric body.
Disclosures: Khandokar Talib indicated no relevant financial relationships. Ahmed Shehadah indicated no relevant financial relationships. Usama Sakhawat indicated no relevant financial relationships. Khadija Raza indicated no relevant financial relationships. Godson Senyendo indicated no relevant financial relationships. Rahat Elahi indicated no relevant financial relationships. Minhaz Ahmad indicated no relevant financial relationships. Ali Marhaba indicated no relevant financial relationships.
Khandokar A. Talib, MD1, Ahmed Shehadah, MD2, Usama Sakhawat, MD3, Khadija Raza, MD3, Godson Senyendo, MD4, Rahat Elahi, 5, Minhaz Ahmad, MD1, Ali Marhaba, MD4. P2103 - Air in the Wrong Places, But the Right Time: Conservative Management of Gastric Pneumatosis and Portal Venous Gas, ACG 2025 Annual Scientific Meeting Abstracts. Phoenix, AZ: American College of Gastroenterology.

 photo")